https://dx.doi.org/10.24016/2026.v12.478
ORIGINAL ARTICLE
Life satisfaction and
perceived overload as predictors of mental health in caregivers of psychiatric
patients in the Peruvian Andes: A cross-sectional study
Jorge Antonio Calderon Apaza 1, Paul Cristian Alanocca Quispe
1
1 Universidad Peruana Unión, Juliaca, Peru.
* Correspondence: jorge.calderon@upeu.edu.pe
Received: September 03, 2025 | Revised:
December 27, 2025 | Accepted: January 25, 2026 | Published Online: January 26, 2026.
CITE IT AS:
Alanocca Quispe, P., Calderon Apaza, J. (2026). Life
satisfaction and perceived overload as predictors of mental health in
caregivers of psychiatric patients in the Peruvian Andes: A cross-sectional
study. Interacciones,
12, e478. https://doi.org/10.24016/2026.v12.478
ABSTRACT
Introduction: Caregivers of psychiatric patients in the Peruvian Andes face unique
challenges where most people do not receive the necessary health care.
Objective: To analyze the association of life satisfaction and perceived competence
with mental health, determining their incremental explanatory contribution
after controlling for sociodemographic variables and perceived overload.
Method: Cross-sectional study with 102 informal caregivers (85.3% women)
recruited in four Community Mental Health Centers in Puno, Peru. Mental health
(MHI-5), overload (Zarit), life satisfaction (SWLS), and sociodemographic
variables were measured. A hierarchical linear regression analysis with
bootstrapping (5000 samples, BCa) was performed to
handle data non-normality, in addition to non-parametric comparisons
(Kruskal-Wallis).
Results: The final model explained 48.5% of the variance (R² adjusted = .48).
Through bootstrapping, life satisfaction (β =0.41, p <.001) and perceived
competence (β=−0.27, p=.004) showed robust significant associations with mental
health. A displacement effect was observed where overload, significant in the
first model, lost statistical significance (p =.103) upon introducing
psychological resources. Likewise, a low level of instruction (primary and
secondary) remained a significant risk factor compared to higher education.
Conclusion: Self-perception of competence and life satisfaction act as protective
factors that displace the direct impact of perceived overload.
Keywords: Mental health; Life satisfaction; Perceived burden; Caregivers.
INTRODUCTION
Caregivers in Latin America continue to exhibit alarming health
conditions, as they are a valuable yet vulnerable resource (Gaviria et al.,
2023; Montorio et al., 1998). Given that mental health lies in the affective
component of emotions and mood, while the life satisfaction section is a
global, cognitive judgment process in which the individual evaluates the
quality of their existence based on their own criteria and internal standards.
They are forced to reorganize their life and adapt them to the needs of the
dependent, facing a double burden of responsibilities that lead them to assume
new physical, psychological, economic, material, and social demands
(Hernandez-Beltran & Bonilla-Farfan, 2024). Added to this, mental disorders
are found to be the primary disability in the world, as one in eight people
suffers from some mental disorder (World Health Organization [WHO], 2022). Just
in Peru, cases of mental dysfunctions are more than 13 million, with a growing
attention in anxiety (18.81%), depression (13.66%), and Psychological
disorders (14.94%) (Ministry of Health [MINSA], 2025). Moreover, Puno is the
second department in Peru with the most significant care gap, with 89.2% of
people receiving low care, meaning that out of every 10 people, 7 do not
receive the care they require (Defensoría del Pueblo,
2025).
The growth of this problem generates a significant segment of dependent
patients, consequently, the need for more caregivers; however, the majority of
these people lack access to constant and effective care, leading to this labor
being occupied more frequently part by part by family members (Oleas et al.,
2024), who often assume this role without the knowledge or necessary skills,
remaining vulnerable to emotional distress due to drastic changes in their
life, thus affecting their well-being and emotional balance (Peng et al.,
2023). The evidence collected in a Colombian meta-analysis helps us dimension
the problem in similar sociocultural contexts, where 53% of caregivers
experience overload, with 31% at a severe level. Said study profiles the
informal caregiver as a woman (85%) between 18 and 60 years old, who assumes
this responsibility alone (61%), often in conditions of economic vulnerability
(65% in a situation of poverty or extreme poverty) and without access to formal
employment (85%) (Gaviria et al., 2023). In defining the term, informal
caregivers are people who care for someone in their social network, voluntarily
and without direct remuneration (Muñoz et al., 2020; Rogero, 2010). These new
changes and responsibilities are not distributed equitably, thus generating a
primary caregiver, who is the most vulnerable piece of the chain; for this
reason, they are denominated as a silent patient, as they accumulate physical
and psychological ailments, which hide behind the demands of the sick family
member (Tripodoro et al., 2015).
As precedent evidence to this study, the following investigations are
presented as research antecedents. In Asia, the predictability of overload on
the quality of life of 459 caregivers of people with mental illnesses was
investigated, through intermediate variables (anxiety, depression, and
self-esteem), finding a significant relationship of overload to the evaluated
quality of life domains (mental health R² = 0.61, and environment R² = 0.41
social relationships R² = 0.35) demonstrating a high explanatory capacity in
the physical and psychological domains; furthermore, it was identified that
caregivers of schizophrenic patients had a lower quality of life compared to
the rest of disorders (bipolar disorders, severe depression), (Cheng et al.,
2022). Within this line of studies performed, 825 informal caregivers from 6
different countries in Europe were surveyed, the result of the sample of
quality of life related to caregiver health was inversely correlated with
overload with a coefficient (r = -0.180;p< 0.001) evidencing that the
greater the caregiver overload, the lower the quality of life (Valcárcel et
al., 2022). In Valencia, Spain, similar results were found when evaluating 136
primary caregivers; 65.5% of the sample presented elevated levels of overload
affecting mainly psychological health, among the other means evaluated
(physical health, mental health, social relationships, and environment)
(Gallardo et al., 2023). Likewise, within a study in Italy, 91 caregivers of
patients with cognitive disorders and motor disabilities were evaluated, within
this it was found that the most significant predictor among the variables (life
satisfaction, resilience, and depression) of perceived overload was life
satisfaction (β = -0.51, R2 = 0.31) which explained 31% of the variance index
(Fianco et al., 2015). In Germany, 489 informal caregivers were evaluated,
seeking to compare the differences between mental health, quality of life, and
care overload, between genders during the second wave of COVID 19 when caring for
patients ≥60 years; with significant statistical differences in women regarding
men in symptoms: depressive (β = 1.00,p< 0.05), anxious (β = 1.38,p<
0.01), of overload (β = 2.00,p< 0.05) and quality of life (β = −2.16,p<
0.01), finding that women were more prejudiced in their care labor in this
period (Zwar et al., 2023). Thus, a significant correlation is observed between
the patient's degree of dependence and the caregiver's level of overload, as
registered in Cuba, where 68% of caregivers showed being severely overloaded
when caring for totally dependent people (p < 0.05) (Gómez et al., 2024).
This implies that the greater the patient's dependence, the fewer of their
needs the informal caregiver can cover (Duran et al., 2024; Ramos et al.,
2023). On the other hand, Hajek and König (2018) did not find a significant
associative relationship between the start of informal care and the mental
health of caregivers, in their study performed in Germany on 13,300 caregivers;
however, an association was found with their life satisfaction (β = −0.14,p< 0.001).
On the other hand, in Latin America, an investigation was performed in
Nuevo León, Mexico on 210 informal caregivers (family members), significant
negative correlations were found between overload and quality of life (r =
-0.314), physical well-being (r = -0.337), psychological (r = -0.388) and
social (r = -0.287) each element with a significance level (p < 0.001) that
is to say, it presents a moderate and negative relationship between quality of
life and its dimensions (Marroquín et al., 2023). In Nivea, Colombia, 68
caregivers participated in a study that found a low, statistically significant
relationship between overload and well-being: physical (r = 0.333),
psychological (r = -0.122), and social (r = 0.541) (Cantillo et al., 2022).
Also in Buenos Aires, Argentina, a study was performed in which overload was
evaluated in 64 primary caregivers, the quality of life and their coping
strategies, in which a significant negative correlation was evidenced between
overload and the dimension of psychological health (r = -.38; p = 0.002) (Hauché et al., 2025).
For this study purpose, a psychiatric patient is someone with a
diagnosed mental disorder whose severity, persistence, and functional impact
place them in a severe or grave category (Pina et al., 2024). This excludes
personality disorders (except schizotypal), substance abuse, disorders without
psychotic symptoms, eating disorders, and recurrent depression (UK National
Health Service [NHS], 2024). To furthermore clarify the conceptual mechanisms
and justify the selection of variables, a theoretical Directed Acyclic Graph
(DAG) is presented (Figure 1). Where the variables influential to Mental health
are hypothesized. In response to the need for parsimony, Life Satisfaction was
prioritized over broader constructs like 'Quality of Life'; as it is a global
construct that houses different thematic fields (Ramirez et al., 2019); while
Life Satisfaction represents the specific cognitive judgment (Baghino & Cortelletti, 2021);
which directly mediates the impact of external circumstances (Overload) on
Mental Health. Likewise, other factors like self-esteem and being dependent on
external feedback are exposed to short-term fluctuations (Hank & Baltes,
2019), making their evaluation in relation to mental health difficult.
Sociodemographic variables that did not show direct theoretical relevance in
the context of the clinical sample studied were omitted.
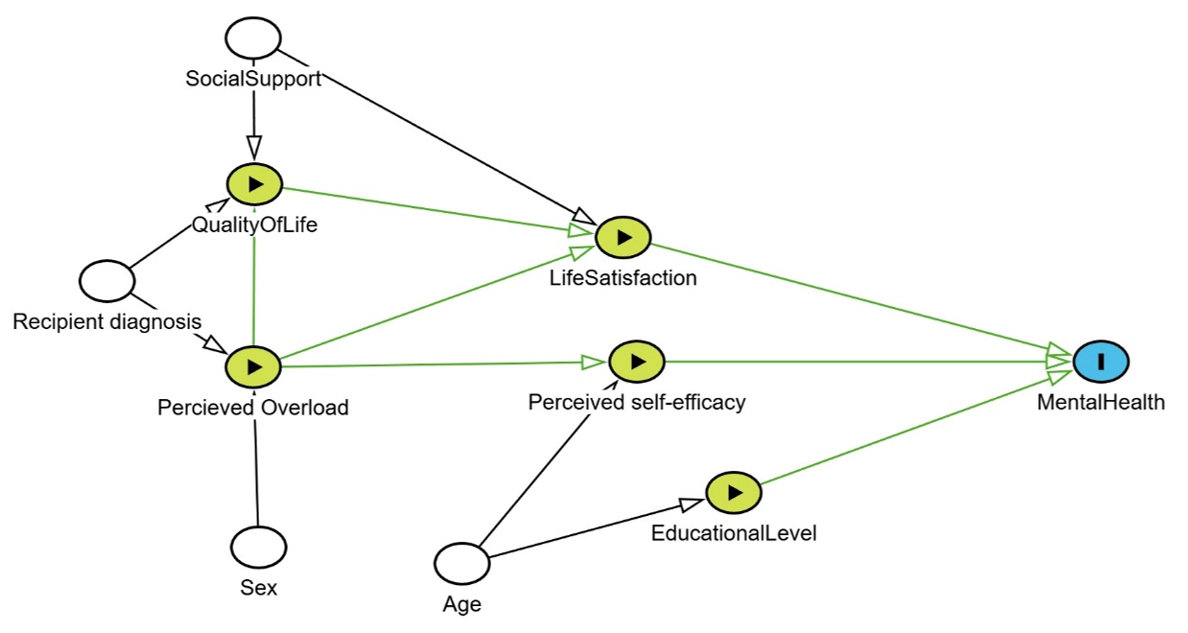
Figure 1. Directed
acyclic graph.
Note: The nodes represent the variables observed in the
study. The green arrows indicate the direct causal trajectories estimated in
the regression model.
Despite the growing importance of mental health, previous evidence, both
national and international, on the subject has not addressed the joint
interaction of our variables as factors associated with the psychological
well-being of caregivers. Added to that, most of these investigations focus on
caregivers of people dependent due to physical disabilities, where overload is
addressed as a purely global construct. In this way, research on caregivers of
people with severe mental disorders is limited, especially in Perú, where
current articles on the subject are scarce. This research contributes a new
perspective by analyzing caregivers of psychiatric patients in the Andean
context of low resources, demonstrating through a hierarchical analysis that
the self-perception of competence possesses a displacement effect on overload,
which will allow a deeper and more updated understanding of the dynamics of
life satisfaction, perceived overload, and mental health in caregivers. This
reorients clinical intervention priorities in the region: programs should not
focus solely on care overload, but predominantly on skills training and
cognitive reinforcement of life satisfaction to shield the caregiver's mental
health.
In this way, the research had as a general objective, to analyze the
association of Life Satisfaction and Perceived Competence with Mental Health,
determining their incremental explanatory contribution when controlling for the
effect of the Degree of Instruction, the Patient's Diagnosis, and Perceived
Overload; and as specific objectives: To evaluate the initial association of
sociodemographic variables (degree of instruction and patient's diagnosis) and
perceived overload with the caregiver's mental health; To determine the
incremental explanatory contribution of psychological resources (life
satisfaction, competence, and interpersonal relationships) in the variance of
mental health, and To compare the levels of mental health, overload, and
psychological resources according to the diagnosis of the care receiver
(Schizophrenia, ASD, and others) to identify significant differences between
groups.
METHODS
Design
The study is developed using a quantitative approach, with a
non-experimental, cross-sectional design. It is framed within an
associative-predictive strategy, as defined by Ato et al. (2013), since it
seeks to estimate the degree of association between a criterion variable and
multiple independent variables.
Participants
The population consists of 102 caregivers of users with open or current
medical records at the 4 community mental health centers operating in Juliaca in 2025. Data was collected between May and July,
with authorization from the network coordination and the heads of each center.
Inclusion criteria used were (full-time or part-time caregivers of dependent
people due to a diagnosed psychiatric disorder, of both sexes; caregivers who
have reached the age of majority, 18 years; having provided care to the user for
at least 3 months; and having informed consent); as exclusion criteria, it was
established: (That the caregiver has some permanent or temporary disability
that prevents answering the tests' questions coherently, having cared for the
user for less than 3 months; patient receives less than 2 psychotherapeutic
sessions per month; patient does not have a psychiatric diagnosis).
To calculate the minimum sample size necessary for the theoretical
model, the software G*Power 3.1.9.7 (Faul et al., 2009) was used with the
following parameters (f²) = 0.35, (α) = 0.05, (1- β) = 0.95, N° predictors 10,
obtaining a minimum required participants of 77; which allows performing the
study with sufficient statistical significance (Cohen, 1992). Thus, the sample
was estimated by a non-probabilistic convenience sampling, based on the
researchers' selection criteria and resources (Otzen & Manterola, 2017).
Variables
The consequences of living with a person affected by some severe
illnesses are known as "care overload" or "family burden",
which encompasses the subjective and objective conditions the caregiver goes
through (Gulayín, 2022). Perceived overload is a
state of feeling sad, stressed, and constantly frustrated experienced by a
caregiver of someone dependent, as this definition encompasses not only the
clinical field but also the social and economic spheres (Márquez et al., 2025).
In the same way, burden refers to emotional and physical health alterations
that occur when demands exceed available resources (Sánchez et al., 2016).
On the other hand, the Pan American Health Organization (2023) states
that mental health is a state of emotional well-being that enables people to
face difficult moments in life through the development of skills, which are a
fundamental mechanism for adequate coexistence in a community. Being that
well-being and health are individual capacities. Furthermore, satisfaction is
defined as a mental state, a positive valuation of something. The term
encompasses both this context and that of "enjoyment", integrating
both cognitive and emotional appreciations (Veenhoven,
1994). Under that proposal, life satisfaction is understood as a judgment that
endures in a time-dependent context, in which the person values their
well-being by comparing their standards of living with their current situation
(Calderón et al., 2018). Therefore, satisfaction is important because it
reflects the cognitive equilibrium between adequate achievement and personal
expectations (Mikulic et al., 2019).
Instruments
To evaluate life satisfaction, the questionnaire (SWLS) Satisfaction
With Life Scale was used, created by Diener et al. (1985); due to the need to
measure how satisfied the population is with their life coming to possess
multiple items, this was designed to evaluate the general opinion of life is an
individual to evaluate individual satisfaction; it was based on the concept of
life satisfaction by Shin and Johnson (1978) who define it as: "A global
assessment of a person's quality of life according to their chosen
criteria." Previously validated in various Peruvian studies, including
that of Calderón et al. (2018), which presented adequate goodness-of-fit
indices (GFI = 0.998, RMSEA = 0.073, SRMR = 0.067). Likewise, it has reported
optimal reliability (ω = 0.90) in a population aged 19 to 64 years. Finally, it
indicates that the instrument evaluates in one dimension the satisfaction with
life with a multiple response scale as an ordinal measure of five response
options under the Likert scale: 1 = strongly disagree, 2 = slightly disagree, 3
= neither agree nor disagree, 4 = slightly agree, 5 = strongly agree. In the
present research, internal consistency indices of Cronbach's alpha (α = 0.731)
and McDonald’s omega (ω = 0.740) were obtained.
On the other hand, to evaluate the perceived overload variable, the
Zarit Burden Interview was used, which was originally developed by Zarit et al.
(1980). This has the purpose of explaining how mental, physical health, and
labor and economic aspects are compromised when caring for a sick person with
dementia. In the Peruvian context, it was validated previously in a population
of caregivers with intellectual disability of 398 informal caregivers between
24 and 65 years old. The instrument consists of 15 items across 4 dimensions:
overload, competence, social relationships, and interpersonal relationships.
These items have Likert response options: (0 = Never, 1 = Rarely, 2 =
Sometimes, 3 = Often, 4 = Almost always). Regarding the validity evidence,
goodness-of-fit indices were found (CFI = 0.95, RMSEA = 0.055, TLI = 0.94),
with optimal reliability evidence (ω = 0.740) (Domínguez et al., 2023). For the
current population, internal consistency indices of Cronbach's alpha (α) =
0.863 and McDonald's omega (ω) = 0.866 were obtained.
Finally, to evaluate mental health, the Mental Health scale MHI-5 was
used, the original version created by Berwick et al. (1991), validated in the
Peruvian context in the adult population, between the ages of 17 and 45 years
by Vilca et al. (2022). It is a brief measure composed of five items, with a
Likert-type response format and four options (never, sometimes, often, and
always), where never is worth 0 and always is worth 3. In the adaptation study,
the scale evidenced adequate psychometric properties. In relation to construct
validity, a confirmatory factor analysis was performed, yielding adequate fit
for the proposed unidimensional model (CFI = 0.99, TLI = 0.99, and RMSEA =
0.07). For the present research, internal consistency indices of Cronbach's alpha
(α = 0.773) and McDonald's omega (ω = 0.790) were obtained.
Data analysis
After collecting the data through surveys and individual interviews, the
data were transcribed manually into Microsoft Excel, ensuring that each item
column was correctly coded to the pertinent scales. For data analysis, Jamovi 2.3.28.0 software and JASP 0.95 were used. The
grouped discrete variables were analyzed using measures of central tendency,
dispersion, and distribution (skewness, kurtosis, quartiles, mean, median, and standard deviation). Furthermore, the univariate
normality of the variables was checked under the Kolmogorov-Smirnov test
(Hernández et al., 2014). This suggests a non-normal distribution, as the
significance levels exceed the 0.05 threshold. Given the non-normality in two
variables, Spearman's Rho correlation coefficients were used.
After that, a Hierarchical Linear Regression with Bootstrapping (5000
resamples) of the BCa type was performed to account
for the nonparametric nature of the data. Variables were introduced in two
functional blocks. In Block 1, control variables (Degree of instruction, Care
hours, Patient disorder) and overload were included. In Block 2, psychological
resources (Competence, Life satisfaction, Social and interpersonal
relationships) were added. The categorical variables (Degree of instruction and
Patient diagnosis) were transformed into dummy variables for the regression
analysis, using 'Higher Education' and 'Schizophrenia' as reference categories,
respectively. After that, the change in R2 (ΔR2) were analyzed, additionally,
the assumptions of multiple linear regression were verified as pointed out by
Vila-Baños et al., (2019), including linearity, normality of residuals,
homoscedasticity, independence of errors and absence of multicollinearity of
independent variables; finally, the analysis of unstandardized coefficients was
performed to quantify the predictability between the variables.
Ethical considerations
The present research was submitted to the Ethics Committee of the
Faculty of Health Sciences of the Universidad Peruana Unión for subsequent
approval under resolution N°2025-CEB-FCS – UPeU-075. Furthermore, the
parameters of the Declaration of Helsinki of the World Medical Association
(WMA, 2024) are followed, where human rights in research are held as priority,
safeguarding integrity, health, dignity, privacy, as well as confidentiality of
all participants, reaching a great responsibility as researchers protecting the
obtained information. Only coming to use it for research purposes, this with
the backing of the College of Psychologists of Peru, which according to chapter
10 of the code of ethics and psychological deontology, confidentiality is a
crucial point not to identify the participants, ethnic group or institution,
respecting the autonomy of the respondents and participants through obtaining
informed consent prior to their participation, guaranteeing their understanding
of the study objectives, and their right to refuse or withdraw at any moment
(Colegio de Psicólogos del Perú, 2017).
RESULTS
102 informal caregivers of users of community mental health centers were
surveyed; based on the results, a data matrix inspection was performed prior to
the inferential analysis. No missing values were detected (0% of missing data)
in the study variables, which is attributed to the face-to-face data collection
strategy performed by trained personnel, who verified the completeness of the
questionnaires in situ. The surveyed caregivers had an average age of 39.8 (SD
= 9.79) years, of whom 85.3% are of the female gender, which is equivalent to
(87 caregivers), while 14.7% represent the male gender with (15 caregivers);
the most common patient-caregiver relationship found was that of parents with
78.4% (n=80), followed by siblings 9.8% (n=10), with 11.8% (n=12) being
children, partners, and other immediate family members; on the other hand, the
time of care most found was between 4 to 10 years with 50% (51) followed by 1
to 3 years with 41.2% (n=42), more than 10 years are 3.9% (4). In the degree of
instruction, it was found that 47.1% (n=48) have complete secondary studies,
33.3% (n=40) pursued higher studies, 12.7% (n=13) have complete primary
studies, 1% (n=1) have incomplete primary studies; in the religion section,
86.3% (88) claim to be Catholic, 3.9% (n=4) are Christian, and 2.9% (n=3) are
Adventist. The caregiver's place of residence is 91.2% (n=93) in Juliaca, 8.8.% (n=9) live in other provinces (Moquegua,
Tacna, Arequipa, Moho), finally in the section of dependent's disorders, 38.2%
(n=39) present schizophrenia, 37.3% (n=38) suffer from ASD, 10.8% (n=11) belong
to ADHD, 13.7% (n=14) present other psychiatric disorders.
When distributing the scores of overloads, life satisfaction,
competence, social and interpersonal relationships, according to the care
receiver's diagnosis in three groups: schizophrenia (n = 39), autism spectrum
disorder (ASD, n = 38), and other diagnoses (n = 25), the descriptive analysis
of the variables showed similar average scores. The non-parametric Kruskal
Wallis statistical analysis confirmed that these differences were not
significant regarding the dimensions of: Overload (X² =0.87,p =
.647); life satisfaction (SWLS) (X² = 2.70,p = .259); competence
(X² = 2.11,p = .348) nor social relationships (X² = 3.51,p
= .173); but there were significant variations regarding the interpersonal
relationship with the care receiver (X² = 6.68,p = .035), where
caregivers of people with schizophrenia present the highest average (M = 5.90,
Me = 7), while Other diagnoses presented the lowest levels, being in turn the
most heterogeneous group (M = 3.92, ME = 3, SD = 3.17).
In Table 1, the assumption of normality was calculated through the Z
statistic, obtained by dividing the skewness and kurtosis values by their
respective standard errors. Considering a significant and non-normal deviation
if the value exceeds ±2 (George & Mallery, 2003). Under said criteria, the
variables of mental health, life satisfaction, overload, and social
relationships found normal values in both skewness and kurtosis; however,
deviations from normality were observed in the competence variable, with a
significant negative skewness (Z = -2.27) with a tendency towards high scores;
as well as in the variable of interpersonal relationships, where a significant
negative kurtosis was found (Z = -2.01), suggesting a platykurtic distribution.
Table 1. Table of normality
of variables.
|
|
Skewness |
kurtosis |
||||
|
|
Mean |
SD |
Value |
SE |
Value |
SE |
|
Mental
health |
6.48 |
3.22 |
0.36 |
0.24 |
-0.57 |
0.47 |
|
Life
satisfaction |
13.08 |
3.78 |
0.39 |
0.24 |
0.01 |
0.47 |
|
Overload |
8.45 |
3.40 |
-0.15 |
0.24 |
-0.55 |
0.47 |
|
Competence |
12.32 |
3.97 |
-0.54 |
0.24 |
-0.35 |
0.47 |
|
Social
relationship |
6.03 |
2.88 |
-0.13 |
0.24 |
-0.85 |
0.47 |
|
Interpersonal
relationship |
5.19 |
3.02 |
-0.17 |
0.24 |
-0.95 |
0.47 |
Table 2 shows the correlations among the three variables and dimensions
(overload, competence, social relationships, and interpersonal relationships).
Life satisfaction and mental health show a moderate positive correlation.
Likewise, life satisfaction and mental health correlate inversely with
perceived caregiver overload and its dimensions, indicating that, at higher
levels of life satisfaction and mental health, they are associated with lower
perceptions of caregiver overload, and vice versa.
Table 2. Table of
correlations.
|
|
SWLS |
CI 95% |
Mental
Health |
CI 95% |
|
Mental
health |
0.535 (<
.001) |
0.371 to
0.655 |
– |
– |
|
Overload |
-0.328
(< .001) |
-0.202 to
-0.536 |
-0.265
(< .007) |
-0.122 to
-0.475 |
|
Competence |
-0.345
(< .001) |
-0.175 to
-0.516 |
-0.468
(< .001) |
-0.356 to
-0.645 |
|
Social
relationships |
-0.383
(< .001) |
-0.217 to
-0.547 |
-0.290
(< .003) |
-0.164 to
-0.508 |
|
Interpersonal
relationships |
-0.182
(< .067) |
0.008 to
-0.368 |
-0.395
(< .001) |
-0.225 to
-0.553 |
The five assumptions of regression were considered: linearity,
independence of errors, homoscedasticity, normality, and non-multicollinearity,
all of which were met (Vila et al., 2019).
In Table 3, the first block explained 20.9% of the variance. The
inclusion of the psychological variables in the second block significantly
increased the model's explanatory capacity by an additional 32.5%. The change
in R² (ΔR² = .325, p < .001) was significant, indicating that
the psychological variables contribute an additional 32.5% of unique
explanation to the model.
Table 3. Model
summary.
|
Model |
R |
R square |
R square
adjusted |
RMSE |
|
M1 |
0.455 |
0.207 |
0.166 |
2.939 |
|
M2 |
0.729 |
0.531 |
0.485 |
2.308 |
As observed in Table 4, after applying bootstrapping, in Model 1,
overload was a significant negative predictor (β = -.265; 95% CI BCa [-.446, -.058]; p = .011), indicating that, when
considering only basic variables, greater overload is associated with lower
mental health. Likewise, the degree of instruction showed a considerable
association, with having only completed primary education versus complete higher
education associated with lower mental health (β = -3.251; 95% CI BCa [-5.203, -1.373]; p = .002). In the same way,
having a complete secondary education as the highest educational level
obtained, versus having complete higher education, predicted lower mental
health (β = -1.98; 95% CI BCa [-3.39, -.49]; p =
.001). Upon introducing the psychological resources in Model 2, the caregiver's
degree of instruction emerged as the most robust associated factor, where
caregivers with complete primary education versus those with completed higher
education, presented lower indices of mental health (β = -2.19; 95% CI BCa [-3.75, -.7];p= .004), similar results were
observed when comparing complete secondary education versus complete higher
education (β = -2.09; 95% CI BCa [-3.264, -.99];p<
.001), followed by competence (β = -.27; 95% CI BCa
[-.43, -.08];p= .003) and life satisfaction (β = .41; 95% CI BCa [.26, .55];p< .001). After the inclusion of
these psychological resources, the overload dimension ceased to be
statistically significant (β = -.17; 95% CI BCa
[-.04, .37]; p = .112). The dimensions of Social and Interpersonal
Relationships did not result in significant differences.
Table 4. Hierarchical
Multiple Regression
|
Model |
|
β (CI 95%) |
Bias |
SE |
p |
|
M1 |
(Intercept) |
10.689
(8.298 to 12.572) |
-0.01 |
1089.00 |
< .001 |
|
Overload |
-0.265
(-0.446 to -0.058) |
0.00 |
0.10 |
0.011 |
|
|
Others -
schizophrenia |
-0.507
(-2.093 to 1.043) |
-0.02 |
0.80 |
0.526 |
|
|
ASD -
schizophrenia |
-0.907
(-2.506 to 0.647) |
-71.21 |
0.80 |
0.226 |
|
|
Primary
education - higher education |
-3.251
(-5.203 to -1.373) |
-0.01 |
0.97 |
0.002 |
|
|
High school
- higher education |
-1.983
(-3.389 to -0.487) |
-0.01 |
0.74 |
0.010 |
|
|
M2 |
(Intercept) |
5.959
(2.694 to 9.304) |
0.01 |
1692.00 |
< .001 |
|
Overload |
0.169
(-0.043 to 0.374) |
-0.01 |
0.11 |
0.112 |
|
|
Others -
schizophrenia |
-1.212
(-2.532 to 0.125) |
-0.01 |
0.68 |
0.075 |
|
|
ASD -
schizophrenia |
-1.166
(-2.424 to 0.016) |
-0.01 |
0.62 |
0.053 |
|
|
Primary
education - higher education |
-2.193
(-3.745 to -0.700) |
-0.04 |
0.78 |
0.004 |
|
|
High school
- higher education |
-2.092
(-3.264 to -0.999) |
0.00 |
0.57 |
< .001 |
|
|
SWLS |
0.409
(0.265 to 0.553) |
0.00 |
0.07 |
< .001 |
|
|
Self competence |
-0.274
(-0.432 to -0.083) |
0.00 |
0.09 |
0.003 |
|
|
Social
relationships |
-0.001
(-0.234 to 0.217) |
0.00 |
0.11 |
0.999 |
|
|
Interpersonal
relationship |
-0.153
(-0.369 to 0.093) |
0.01 |
0.12 |
0.192 |
Note:
Bootstrapping based on 5000 samples. Schizophrenia and completed higher
education were used as reference variables.
DISCUSSION
The purpose of this study was to determine the degree of association of
life satisfaction and perceived overload on mental health. For this, a multiple
linear regression model was estimated which explained 48.5% of the variance,
where it was observed that life satisfaction (β = .41; 95% CI BCa [.26, .55];p< .001), the caregiver's self-perception
of competence (β = -.27; 95% CI BCa [-.43, -.08];p=
.003) and the level of instruction, compared between primary education to
completed higher education (β = -2.19; 95% CI BCa
[-3.75, -.7];p= .004) and secondary education to completed higher education (β
= -2.09; 95% CI BCa [-3.264, -.99];p< .001) were
significantly associated with mental health.
Competence showed a negative association regarding mental health (β =
-.27; 95% CI BCa [-.43, -.08]; p= .003). In line with
previous investigations, it was identified that self-efficacy was significantly
related to the mental health of caregivers, β = .10 (p = .001) (Clarke et al.,
2021), as well as negatively to depressive symptoms (β = -1.647; p< .001)
(Tang et al., 2015). Suggesting that, the negative perception a person has
about their capacity to provide care (Albarracín et al., 2016), or the
"competence" factor, is directly associated with their mental health.
Determining their level of motivation and confidence, thus beliefs in personal
capacities can transform apparently threatening situations into manageable
situations, preventing risky behaviors and promoting adaptive behaviors
(Zenteno et al., 2017). On the other hand, under Ellis's parameters, this lack
of confidence in one's own skills would be in irrational beliefs such as
perfectionist expectations (Ellis & Grieger, 1981). These results position
the caregiver's perception of their own capacities as a mechanism strongly
associated with their mental health.
Subsequently, life satisfaction was the second most robust positive
relationship (β = .41; 95% CI BCa [.26, .55];p< .001), which is in line with other studies in
informal caregivers in the Netherlands, where life satisfaction was
significantly associated with psychological well-being (β = .155, p= .016) (Bremmers et al., 2024). That suggests that life
satisfaction, which is the comparison between the individual's subjective
standard and their personal circumstances (Diener et al., 1985), acts as a
positive psychological resource for the caregiver; in other words, maintaining
standards close to their current life condition (Calderón et al., 2018). It
acts as a resilience-promoting factor (WHO, 2022), making life satisfaction a
significant and protective factor for the mental health of caregivers.
The caregiver's level of instruction was negatively and significantly
associated with mental health when comparing completed higher education
(reference group) against completed primary education (β = -2.19; 95% CI BCa [-3.75, -.7];p= .004) and against completed secondary
education (β = -2.09; 95% CI BCa [-3.264, -.99];p<
.001), evidencing that caregivers with a lower educational level are associated
with worse mental health. In the same line of research, there are precedents
that the highest educational level obtained acts as a protective factor against
various disorders, such as major depression, alcohol dependence, generalized
anxiety, ADHD, and PTSD (Demange et al., 2024), for it is associated with
better cognitive skills, emotional regulation and cooperation which is linked
to better mental health (Jareebi et al., 2024). This
phenomenon is especially seen in women of primary or lower educational levels
since they are 86% more prone to suffering anxious or depressive disorders (Bacigalupe et al., 2020).
Finally, the non-significance of the overload score in our final model
is of particular interest (β = -.17; 95% CI BCa
[-.04, .37]; p= .112), for it disagrees with similar studies, where the
overload coefficient on mental health or psychological well-being was: β =
-.40, p< .001 (Nah et al., 2022). β = -.294, p< .001 (Bremmers
et al., 2024) β = -.262; p= .001 (Agyemang et al., 2024). Furthermore,
literature on caregiver well-being has consistently established overload as a
variable related to negative results in mental health or psychological
well-being, as it is associated with symptoms of sadness, feelings of burden,
and stress (Marquéz, 2025). In our results, a
displacement effect is observed due to the statistical control of variables
(Becker, 2005). While in the first model a significant negative association was
observed between overload and mental health (β = -.264; 95% CI BCa [-.45, -.06]; p = .017), the effect disappeared upon
introducing the other psychological resource variables (p = .112). Especially
the "competence" variable, which, due to its specificity, seems to
capture the variance associated with mental health that, otherwise, would be
attributed to overload. This relationship is not commonly explored due to
methodological limitations rooted in the original Zarit test's global overload
score (Zarit et al., 1980), and it does not imply that care overload is
irrelevant; instead, it suggests that the caregiver's perception of competence
is a more robust protective factor. This theoretical model would explain why a
direct relationship between providing informal care and the caregiver's mental
health is not always found (Hajek and König, 2018).
Limitations
and strengths
The present study must be interpreted considering the methodological
limitations presented. The cross-sectional design prevents the observation of
variables over time; furthermore, an influence of third variables, mediating
variables, or reverse directionality not measured cannot be ruled out;
furthermore, the selection of the sample being non-probabilistic by convenience
limits generalizing findings to the general population of caregivers of the
region (Etikan et al., 2016). At the same time, the
selection bias inherent to intrahospital recruitment is recognized, considering
a regional mental health care gap of 89.2% (Defensoría
del Pueblo, 2025), which excludes caregivers without access to the formal
system. Likewise, the instruments (SWLS, Zarit, and MHI-5) have national
validation; the lack of specific adaptation to the Andean context could
introduce cultural or linguistic biases in the local population's
interpretation of the items.
Just as the mentioned limitations, the study also possesses several
notable strengths; the main one is the analytical approach that allows the
deconstruction of the concept of overload, since the version of the Zarit
instrument by Albarracín et al. (2016) does not measure overload as a global
construct. However, as a further dimension, by isolating its components, we
managed to discern which exerts the greater effect within the proposed model,
offering a view of the specific psychological mechanism of association, moving
away from the traditional approach predominant in the literature. On the other
hand, data collection was conducted by trained personnel in a face-to-face and
individual manner, ensuring the quality of the collected information.
Recommendations
Based on the results, it is recommended that interventions for
caregivers of psychiatric patients focus on strengthening perceptions of
competence, increasing life satisfaction, and facilitating access to
educational opportunities. At an individual level, caregivers must receive
practical, continuous training that helps them feel secure in their role, as
well as psychological support and self-care spaces that enhance their overall
well-being. For researchers, beyond the direct relationships between competence
and mental health and between life satisfaction and mental health, it would be
helpful to investigate variables that mediate or moderate those relationships.
On the other hand, public entities should implement accessible training
programs, create emotional support networks, and offer services that foster a
balance between personal life and care. Finally, at the level of public
policies, it is proposed to formally recognize the caregiver's role, develop
interventions centered on the improvement of perceived competence and life
satisfaction, and include indicators like life satisfaction and perception of
competence in institutional evaluations, to ensure integral and sustainable
accompaniment of those who fulfill this essential labor in the mental health system.
Conclusions
The results of this study indicate that the mental health of caregivers
in the sample studied is strongly associated with their level of instruction,
life satisfaction, and self-perception of competence, and the final model
presented explained 48.5% of the variance.
ORCID
Jorge Antonio Calderon Apaza: https://orcid.org/0009-0005-9615-004x
Paul Cristian Alanocca Quispe: https://orcid.org/0000-0002-0881-4610
AUTHORS’
CONTRIBUTION
Jorge Antonio Calderon Apaza: Manuscript
conception; Data collection; Data analysis and interpretation; Manuscript
writing.
Paul Cristian Alanocca
Quispe: Manuscript conception; Data collection; Data analysis and
interpretation; Manuscript writing.
FUNDING SOURCE
This paper was self funded and supported by “Universidad Peruana Unión” in
collaboration with “Red de salud San Roman”.
CONFLICT OF INTEREST
The authors declare that there were no conflicts of
interest in the collection of data, analysis of information, or writing of the
manuscript.
ACKNOWLEDGMENTS
Not applicable.
REVIEW PROCESS
This study has been reviewed by two external reviewers in double-blind
mode. The editor in charge was David Villarreal-Zegarra. The review process is included
as supplementary material 1.
DATA AVAILABILITY STATEMENT
The authors attach the
database as supplementary material 2.
DECLARATION OF THE USE OF GENERATIVE ARTIFICIAL INTELLIGENCE
We used DeepL to translate specific sections of the manuscript and
Grammarly to improve the wording of certain sections. The final version of the
manuscript was reviewed and approved by all authors.
DISCLAIMER
The authors are responsible for all statements made in this article.
REFERENCES
Albarracín Rodríguez, Á., Cerquera Córdoba, A., & Pabón
Poches, D. (2016). Escala de sobrecarga del cuidador Zarit: Estructura
factorial en cuidadores informales de Bucaramanga. Revista de Psicología
Universidad de Antioquia, 8(2), 87–99. https://doi.org/10.17533/udea.rpsua.v8n2a06
Agyemang-Duah, W., Oduro, M. S., Peprah,
P., Adei, D., & Nkansah, J. O. (2024). The role of gender in health
insurance enrollment among geriatric caregivers: results from the 2022 informal
caregiving, health, and healthcare survey in Ghana. BMC Public Health, 24(1),
1566. https://doi.org/10.1186/s12889-024-18930-y
Asociación Médica Mundial. (2024). Declaración de Helsinki. http://www.wma.net/s/ethicsunit/helsinki.htm
Ato, M., López, J. J., & Benavente, A. (2013). Un sistema de
clasificación de los diseños de investigación en psicología. Anales de
Psicología, 29(3), 1038-1059. https://doi.org/10.6018/analesps.29.3.178511
Bacigalupe,
A., Cabezas, A., Bueno, M. B., & Martín, U. (2020). El género como
determinante de la salud mental y su medicalización. Informe SESPAS 2020.
Gaceta sanitaria, 34, 61-67. https://doi.org/10.1016/j.gaceta.2020.06.013
Baghino,
D., & Cortelletti, L. (2021). Satisfacción vital
y felicidad en primera y seguna ola de la pandemia
por COVID-19. Anuario de Investigaciones, 28(1), 339–346.
Becker, T. E. (2005). Potential problems in the
statistical control of variables in organizational research: A qualitative
analysis with recommendations. Organizational research methods, 8(3),
274-289.
Berwick, M., Murphy, M., Goldman, A., Ware, E.,
Barsky, J., & Weinstein, C. (1991). Performance of a Five-Item Mental
Health Screening Test. Medical Care, 29(2), 169–176. https://doi.org/10.1097/00005650-199102000-00008
Bremmers, L. M., Fabbricotti, I. N., & Hakkaart,
L. (2024). The impact of informal care provision on the quality of life of
adults caring for persons with mental health problems:
A cross-sectional assessment of caregiver quality of life. SAGE Open Nursing, 10. https://doi.org/10.1177/20551029241262883
Calderón-De la Cruz, G., Lozano Chávez, F., Cantuarias Carthy, A.,
& Ibarra Carlos, L. (2018). Validación de la Escala de Satisfacción con la
Vida en trabajadores peruanos. Liberabit,
24(2), 249-264. https://doi.org/10.24265/liberabit.2018.v24n2.06
Cantillo-Medina, P., Perdomo-Romero, Y., & Ramírez-Perdomo, A.
(2022). Características y experiencias de los cuidadores familiares en el
contexto de la salud mental. Revista Peruana de Medicina Experimental y
Salud Pública, 39(2), 185-192. http://doi.org/10.17843/rpmesp.2022.392.11111
Cheng, C., Chang, C. S., Griffiths, M. D., Yen, C. F.,
Liu, H. C., Su, J. A., Lin, C. Y., & Pakpour, A.
H. (2022). Quality of life and care burden among family caregivers of people
with severe mental illness: Mediating effects of self-esteem and psychological
distress. BMC psychiatry, 22(1), 672. https://doi.org/10.1186/s12888-022-04289-0
Clarke, R., Farina, N., Chen, L., Rusted, M., &
IDEAL program team. (2021). Quality of life and well-being of carers of people
with dementia: are there differences between working and nonworking carers?
Results from the IDEAL program. Journal of Applied Gerontology, 40(7),
752-762. https://doi.org/10.1177/0733464820917861
Cohen, J. (1992). A power primer. Psychological
Bulletin, 112(1), 155–159. https://doi.org/10.1037/0033-2909.112.1.155
Colegio de Psicólogos del Perú. (2017). Código de Ética y Deontología Profesional. Colegio de Psicólogos del Perú.
Defensoría del Pueblo. (2025, 10 de octubre). Defensoría del
Pueblo reitera necesidad de fortalecer la Dirección de Salud Mental para
superar las brechas en materia de atención a pacientes. https://www.defensoria.gob.pe/defensoria-del-pueblo-reitera-necesidad-de-fortalecer-la-direccion-de-salud-mental-para-superar-las-brechas-en-materia-de-atencion-a-pacientes/
Demange, P. A., Boomsma, D. I., van Bergen, E., &
Nivard, M. G. (2024). Evaluating the causal relationship between educational
attainment and mental health. medRxiv, 2023-01. https://doi.org/10.1101/2023.01.26.23285029
Diener, E., Emmons, R., Larsen, R., & Griffin, S.
(1985). The Satisfaction with Life Scale. Journal of Personality Assessment,
49(1), 71-75. https://doi.org/10.1207/s15327752jpa4901_13
Domínguez, J., Santa-Cruz, H., & Chávez, V.
(2023). Zarit Caregiver Burden Interview: Psychometric Properties in Family
Caregivers of People with Intellectual Disabilities. Eur. J. Investig. Health Psychol. Educ., 13(2), 391-402. https://doi.org/10.3390/ejihpe13020029
Duran, T., Llorente, Y., & Romero, I. (2024). Dependencia funcional del receptor del cuidado, sobrecarga y
calidad de vida del cuidador de personas con tratamiento sustitutivo renal. Revista
Salud Uninorte, 40(2), 416-430. https://doi.org/10.14482/sun.40.02.357.753
Ellis, A., & Grieger, R. M. (Eds.).
(1981). Manual de terapia racional-emotiva (Vol. 1). Desclée De Brouwer.
Etikan, I., Musa, S. A., & Alkassim, R. S. (2016). Comparison of convenience
sampling and purposive sampling. American Journal of Theoretical and Applied
Statistics, 5(1), 1–4. https://doi.org/10.11648/j.ajtas.20160501.11
Faul, F., Erdfelder, E., Buchner, A., & Lang,
A.-G. (2009). Statistical power analyses using G*Power 3.1: Tests for
correlation and regression analyses. Behavior research methods 41(4),
1149-1160 https://doi.org/10.3758/BRM.41.4.1149
Fianco, A., Sartori, D., Negri, L., Lorini, S., Valle,
G., & Delle Fave, A. (2015). The relationship
between burden and well-being among caregivers of Italian people diagnosed with
severe neuromotor and cognitive disorders. Research in developmental
disabilities, 39, 43-54. https://doi.org/10.1016/j.ridd.2015.01.006.
Gallardo J., Bravo , J., Gallego, J., & Guitiérrez, J.
(2023). Calidad de vida y sobrecarga en el
cuidador principales. Journal Nursing, 2952-3192.
Gaviria, D., Moreno, S., & Díaz, L. (2023). Sobrecarga del
cuidador familiar en Colombia: revisión sistemática exploratoria. Revista
colombiana de enfermería, 22(1), 17-31. https://doi.org/10.18270/rce.v22i1.3754
Gómez-Soler, U., Hierrezuelo-Rojas, N.,
Hernández-Magdariaga, A., Acosta-Montero, D., Ramos-Isacc, Y., &
Trujillo-Moreno, Y. (2024). Sobrecarga en cuidadores primarios de adultos
mayores dependientes. Archivo Médico Camagüey, 28, e10021.
Gulayín,
M. (2022). Carga en cuidadores familiares de personas con esquizofrenia: una
revisión bibliográfica. Vertex Revista Argentina de
Psiquiatría, 33(155), 50-65. https://doi.org/10.53680/vertex.v33i155.135.
Hank, P., &
Baltes-Götz, B. (2019). The stability of self-esteem variability: A
real-time assessment. Journal of Research in Personality, 79, 143–150. https://doi.org/10.1016/j.jrp.2019.03.004
Hajek, A., & König, H. (2018). The relation
between personality, informal caregiving, life satisfaction and health-related
quality of life: evidence of a longitudinal study. Quality
of Life Research, 27, 1249-1256. https://doi.org/10.1007/s11136-018-1787-6.
Hauché, A., Chiaramonte, A., Galvagno,
G., & Isabel, G. (2025). Sobrecarga,
calidad de vida y estrategias de afrontamiento en cuidadores primarios de
pacientes crónicos. Revista Iberoamericana ConCiencia,
10(1), 42-60. https://doi.org/10.70298/ConCiencia.10-1.5.
Hernández Sampieri, R., Fernández Collado, C., & Baptista
Lucio, P. (2014). Definiciones de los enfoques cuantitativo y cualitativo, sus
similitudes y diferencias. En Metodología de la investigación (6.ª ed., pp.
2-21). McGraw-Hill.
Hernandez-Beltran, K., & Bonilla-Farfan, D. (2024). Percepción
de la carga del cuidador familiar de personas con alteraciones en la salud
mental. Boletín Semillero de Investigación en Familia, 6(1). https://doi.org/10.22579/27448592.1137.
Jareebi, M. A., & Alqassim, A.
(2024). The impact of
educational attainment on mental health: A causal assessment from the UKB and FinnGen cohorts. Medicine, 103(26), e38602. https://doi.org/10.1097/MD.0000000000038602
Márquez, A. (2025). Revisión de la evidencia empírica relacionada
con el síndrome de sobrecarga del cuidador publicada en los últimos diez años. Trabajo
Social Hoy, 103(1), 1-23. https://doi.org/10.12960/TSH.2025.0001
Márquez, V., Calderon, C., & Agustin, E. (2025). Círculo
vicioso de la enfermedad. El nivel de sobrecarga del cuidador primario del
paciente oncológico pediátrico. Salud Publica y enfermedades, 116 - 152.
https://hdl.handle.net/20.500.12866/3973
Marroquín-Escamilla, R., Santos-Flores, M., Montes de Oca Luna,
R., Santos-Flores, I., Obregón Sánchez, N. H., & Trujillo-Hernández, P. E.
(2023). Calidad de vida y sobrecarga de cuidadores familiares en primer nivel
de atención. Revista Salud Uninorte, 40(2), 416-430. https://doi.org/10.14482/sun.40.02.357.753
Mikulic, M., Crespi, M., & Caballero, Y. (2019). Escala de
satisfacción con la vida (SWLS): Estudio de las propiedades psicométricas en
adultos de Buenos Aires. Anuario de investigaciones, 26, 395-402.
Ministerio de Salud. (2025, 10 de
enero). Establecimientos del Minsa atendieron más de 250 000 casos de
depresión a lo largo del año 2024. Plataforma del Estado Peruano. https://www.gob.pe/institucion/minsa/noticias/1088925-establecimientos-del-minsa-atendieron-mas-de-250-000-casos-dedepresion-a-lo-largo-del-ano-2024
Montorio, I., Fernández, M., López., A & Sánchez, M. (1998).
La entrevista de carga del cuidador. Utilidad y validez del concepto de carga. Revista
Psicologica, 229-248.
Muñoz, G., & Enrique, G. (2020). Diseño de un taller para
cuidadores informales de adultos mayores del Servicio de Medicina en Hospital
Dr. Sótero del Río. Revista Vida,
99-109. http://doi.org/10.13140/RG.2.2.12972.48003
National Health Service (NHS). (2024). Quality and
Outcomes Framework (QOF): Guidance for 2024/25. NHS England. https://www.england.nhs.uk/
Nah, S., Martire, L. M., & Zhaoyang,
R. (2022). Perceived gratitude, role overload, and mental health among spousal
caregivers of older adults. The Journals of Gerontology: Series B, 77(2),
295-299. https://doi.org/10.1093/geronb/gbab086
Oleas Rodríguez, D. A., Yong
Peña, C., Garza Olivares, X., Teixeira Filho, F. S., Lucero Córdova, J. E.,
& Salas Naranjo, A. J. (2024). Emotional Coping Strategies for
Informal Caregivers of Hospitalized Patients: A Study of Distress and Overload.
Psychology Research and Behavior Management, 725-734. https://doi.org/10.2147/PRBM.S443200
Otzen, T., & Manterola, C. (2017). Técnicas de Muestreo sobre una Población a Estudio. Int. J. Morphol, 227-232. http://doi.org/10.4067/S0717-95022017000100037
Pan American Health Organization (2023). Salud mental:
https://www.paho.org/es/temas/salud-mental
Peng, Y., Xu, Y., Yue, L., Chen, F., Wang, J., &
Sun, G. (2023). Resilience in informal caregivers of patients with heart
failure in China: exploring influencing factors and identifying the paths. Psychology
Research and Behavior Management, 1097-1107. https://doi.org/10.2147/PRBM.S405217
Pina, S., Kousoulis, A. A.,
& Spandler, H. (2024). ‘Severe mental
illness’: Uses of this term in physical health support policy, primary care
practice, and academic discourses in the United Kingdom. BMC Psychiatry, 24(1), 172. https://doi.org/10.1186/s12888-024-06048-4
Ramírez-Coronel, A. A., Malo-Larrea, A.,
Martínez-Suarez, P. C., Montánchez-Torres, M. L., Torracchi-Carrasco, E., &
González-León, F. M. (2020). Origen, evolución e investigaciones sobre la
Calidad de Vida: Revisión Sistemática. Archivos venezolanos de farmacología y
terapéutica, 39(8), 954-959. https://doi.org/10.5281/zenodo.4543649
Ramos, F., Morales, S., & Henao-Castaño, M. (2023).
Funcionalidad familiar y sobrecarga de cuidador según grado de dependencia del
adulto mayor. Presencia, e14373.
Rogero García, J. (2010). Los
tiempos del cuidado: El impacto de la dependencia de los mayores en la vida
cotidiana de sus cuidadores. IMSERSO.
Sánchez-Herrera, B., Carrillo-González, G. M., Chaparro-Díaz, L.,
Carreño, S. P., & Gómez, O. J. (2016). Concepto carga en los modelos
teóricos sobre enfermedad crónica: Revisión sistemática. Revista de Salud
Pública (Bogotá), 18(6), 976–985. https://doi.org/10.15446/rsap.v18n6.53210
Shin, C., & Johnson, M. (1978). Avowed happiness
as an overall assessment of the quality of life. Social Indicators Research,
5, 475–492. https://doi.org/10.1007/BF00352944
Tang, F., Jang, H., Lingler,
J., Tamres, L., & Erlen, J. (2015). Stressors and
caregivers’ depression: Multiple mediators of self-efficacy, social support,
and problem-solving skill. Social Work in Health
Care, 54(7), 651–668. https://doi.org/10.1080/00981389.2015.1054058
Tripodoro, V. A., Veloso, V., & Llanos, V. (2015). Sobrecarga del cuidador principal de pacientes en cuidados
paliativos. Argumentos. Revista de Crítica Social, (17), 213-231.
Valcárcel-Nazco, C., Ramallo-Fariña, Y., Linertová,
R., Ramos-Goñi, M., García-Pérez, L., & Serrano-Aguilar, P. (2022). Health-Related Quality of Life and Perceived Burden of
Informal Caregivers of Patients with Rare Diseases in Selected European
Countries. International Journal of Environmental Research and Public
Health, 19(13), 8208. https://doi.org/10.3390/ijerph19138208.
Veenhoven, R. (1994). El estudio de la satisfacción con la vida. Intervención
Psicosocial, 3(8), 87-116. http://hdl.handle.net/1765/16195
Vilà-Baños,
R., Torrado-Fonseca, M., & Reguant-Alvarez, M.
(2019). Análisis de regresión lineal múltiple con SPSS: Un ejemplo práctico. REIRE
Revista d'Innovació i Recerca en Educació,
12(2), 1-10.
Vilca, L., Chávez, B., Fernandez, Y.,
& Caycho, T. (2022). Spanish
version of the revised Mental Health Inventory-5 (R-MHI-5): New Psychometric
Evidence from the Classical Test Theory (CTT) and the Item Response Theory
Perspective (IRT). Trends in Psychology, 30, 111-128. https://doi.org/10.1007/s43076-021-00107-w
World Health Organization (2022). Salud Mental; fortalecer nuestra respuesta. Organización Mundial
de la Salud. https://www.who.int/news-room/fact-sheets/detail/mental-health-strengthening-our-response.
World Health Organization (2025, 30 de septiembre). Mental disorders. https://www.who.int/news-room/fact-sheets/detail/mental-disorders
Zarit, S. H., Reever, K. E., & Bach-Peterson, J.
(1980). Relatives of the impaired elderly: Correlates of feelings of burden. The
Gerontologist, 20(6), 649–655. https://doi.org/10.1093/geront/20.6.649
Zenteno, A., Cid, P., & Saez, K. (2017). Autoeficacia del cuidador familiar de la persona en estado
crítico. Enfermería Universitaria, 14(3), 146–154. https://doi.org/10.1016/j.reu.2017.05.001
Zwar, L., König, H., & Hajek, A.
(2023). Gender differences in
mental health, quality of life, and caregiver burden among informal caregivers
during the second wave of the COVID-19 pandemic in Germany: A representative,
population-based study. Gerontology, 69(2), 149-162. https://doi.org/10.1159/000523846