https://dx.doi.org/10.24016/2026.v12.519
ORIGINAL ARTICLE
LGBT Moral Injury Scale: Initial Validation and Preliminary Psychometric
Properties
Juan Aníbal González-Rivera 1*, Adam Rosario-Rodríguez 2
1 School of
Behavioral and Brain Sciences, Ponce Health Sciences University, Puerto Rico,
United States of America.
2 Albizu University,
San Juan Campus, San Juan, Puerto Rico, United States of America.
* Correspondence: jagonzalez@psm.edu
Received: February 18, 2026 | Revised: March 19, 2026 | Accepted:
March 29, 2026 | Published Online: June 03, 2026.
CITE IT AS:
González-Rivera, J. A., & Rosario-Rodríguez, A.
(2026). LGBT
Moral Injury Scale: Initial Validation and Preliminary Psychometric Properties.
Interacciones, 12, e519. https://doi.org/10.24016/2026.v12.519
ABSTRACT
Background: Moral injury has been linked to guilt, shame,
self-condemnation, and moral disorientation; however, existing measures have
been developed primarily in military, veteran, or healthcare contexts and may
not adequately capture identity-related moral suffering in LGBTQ+ populations.
Objective: To develop the LGBT Moral Injury Scale (LGBT-MIS) and
provide initial psychometric evidence for its use with LGBTQ+ adults in Puerto
Rico.
Method: A total of 242 LGBTQ+ adults were recruited through
social media and snowball sampling. Because multivariate normality was
violated, we conducted confirmatory factor analyses using robust estimation to
compare a unidimensional model, a theory-driven five-factor model, and refined
alternative models. We evaluated global model fit, factor loadings, item
discrimination, internal consistency (α, ω, and composite
reliability), convergent validity (AVE), discriminant validity (ASV, MSV), interfactor correlations, and external convergent
associations with PTSD symptoms and Negative Religious Coping.
Results: The unidimensional model showed poor fit, whereas the theory-driven model demonstrated mixed fit and several loadings below .65. After item refinement, a
15-item, five-factor solution—Guilt, Shame, Moral Conflicts, Religious
Struggle, and Self-Condemnation—showed adequate fit, satisfactory reliability,
and acceptable item discrimination. AVE supported convergent validity, and ASV
supported discriminant validity; however, MSV exceeded AVE for Guilt, Shame,
and Moral Conflicts, indicating partial overlap among these factors. Interfactor correlations were positive and moderate.
Associations with PTSD symptoms and Negative Religious Coping provided initial
evidence of external convergent validity.
Conclusions: The LGBT-MIS provides promising initial support as a
multidimensional measure of moral injury in Puerto Rican LGBTQ+ adults. With
further validation, the scale may support research and clinically informed
assessment of guilt, shame, moral conflict, religious struggle, and
self-condemnation in LGBTQ+ populations.
Keywords: moral injury, LGBTQ+, minority stress, psychometrics,
religious struggle, validity
INTRODUCTION
Moral injury is a complex psychological construct
referring to the deep distress that arises when an individual perceives a
transgression of their core moral beliefs and values, resulting in profound
feelings of guilt, shame, self-condemnation, and moral disorientation (Griffin
et al., 2019). Originally described in the context of military personnel and
veterans exposed to morally injurious events such as combat-related actions or
betrayals, moral injury has been increasingly recognized as a distinct and clinically
significant phenomenon with substantial impact on mental health outcomes,
including posttraumatic stress disorder (PTSD), depression, and suicidal
ideation (Koenig et al., 2019; Maguen et al., 2022).
Although most research on moral injury has focused on
military populations, recent scholarship highlights the relevance of this
construct to marginalized groups experiencing chronic social and
identity-related stressors, including sexual and gender minorities (SGM), often
referred to collectively as the LGBTQ community (Nicholson et al., 2025). This
population faces unique and persistent minority stressors, such as
discrimination, stigma, rejection by family or community, and internalized
homonegativity, which can serve as potentially morally injurious events (PMIEs)
(Nicholson et al., 2025; Ren et al., 2018). These experiences challenge
fundamental moral and identity beliefs and can elicit intense emotions of
shame, guilt, and internal conflict, which are central elements of moral injury
(Nicholson et al., 2025).
The minority stress model provides a valuable
explanatory framework, elucidating how distal stressors (external
discrimination and prejudice) and proximal stressors (identity concealment,
internalized stigma) cumulatively exacerbate psychological distress among LGBTQ
individuals (Nicholson et al., 2025; Herron, 2020). Empirical evidence
substantiates associations between exposure to PMIEs and adverse mental health
outcomes in this group, such as increased rates of anxiety, depression,
substance use, PTSD symptoms, and suicidal behavior (Griffin et al., 2019;
Mantri et al., 2020). These findings call for a nuanced understanding of moral
injury beyond trauma-exposed military cohorts, with a culturally sensitive lens
attentive to the lived experiences of LGBTQ people.
In LGBTQ+ populations, moral injury may arise not only
from discrete potentially morally injurious events but also from chronic
exposure to social and structural conditions that frame one’s identity as
wrong, sinful, unacceptable, or incompatible with dominant moral expectations
(Herek, 2007; Meyer, 2003; Nicholson et al., 2025). Structural discrimination,
stigmatization, family or community rejection, identity concealment, and
conflict with heteronormative or cisnormative norms
may function as morally injurious experiences when they undermine an
individual’s sense of worth, coherence, and belonging (Herek, 2007; Meyer,
2003). In this sense, moral injury overlaps with, but is not reducible to,
minority stress or psychological trauma. Whereas minority stress theory helps
explain the chronic burden imposed by stigma, prejudice, and internalized
negativity, moral injury highlights the moral-emotional and existential
consequences of these experiences, including guilt, shame, self-condemnation,
spiritual struggle, and moral disorientation (Meyer, 2003; Nicholson et al.,
2025). This distinction is important because it helps justify the need for a
specialized instrument capable of capturing identity-based and socioculturally embedded forms of moral suffering in LGBTQ+
populations (Nicholson et al., 2025).
One particularly salient domain in the LGBTQ moral
injury experience is the dimension of religious and spiritual struggle. LGBTQ
individuals frequently contend with conflicting narratives between their sexual
or gender identity and doctrinal teachings of faith communities, leading to
feelings of divine punishment, abandonment, and spiritual betrayal (Ren et al.,
2018). This internal religious conflict further complicates moral distress and
may contribute to self-condemnation or withdrawal from social support
(Nicholson et al., 2025; Mantri et al., 2020). Conversely, spirituality may
also serve as a source of resilience when integrated affirmatively (Nicholson
et al., 2025).
Despite this growing body of knowledge, there remains
a critical gap in validated psychometric instruments tailored to capture moral
injury as it uniquely manifests in LGBTQ populations. Existing measures of
moral injury, developed for military or healthcare professional contexts, tend
to emphasize domains such as betrayal, guilt, and shame without addressing
identity-specific conflicts, religious struggles, and internalized stigma
typical in LGBTQ cohorts (Mantri et al., 2020). This lack of appropriate assessment
tools limits the capacity for precise identification, research, and development
of tailored clinical interventions.
To bridge this gap, the present study introduces and
psychometrically evaluates the LGBT Moral Injury Scale (LGBT-MIS), a
multidimensional instrument specifically designed for LGBTQ+ populations.
Unlike existing moral injury measures developed primarily for military,
veteran, or healthcare settings, the LGBT-MIS was constructed to assess morally
injurious experiences that emerge within minority-stress contexts and that are
closely tied to sexual and gender identity. Its distinctive contribution lies
not only in assessing core moral emotions such as guilt and shame, but also in
capturing identity-related moral conflicts, religious and spiritual struggle
linked to sexual or gender identity, and self-condemnation associated with
internalized stigma, social invalidation, and rejection. In this way, the
LGBT-MIS extends the assessment of moral injury beyond betrayal- and
transgression-focused models by addressing how chronic discrimination,
concealment, family or community rejection, and conflict with heteronormative
or cisnormative values may function as morally
injurious experiences for LGBTQ+ individuals.
The scale was conceptually organized around five core
dimensions: guilt, shame, moral conflicts, religious struggle, and
self-condemnation. Guilt reflects feelings of having failed familial, cultural,
or societal expectations and self-reproach related to one’s sexual or gender
identity; shame refers to perceived negative social judgment and internal
embarrassment associated with identity; moral conflicts capture the internal
struggle of reconciling one’s authentic self with dominant social and moral norms;
religious struggle addresses spiritual pain, alienation, and questions about
divine justice in response to identity-related condemnation; and
self-condemnation refers to harsh self-evaluation, self-blame, and diminished
self-worth. Together, these dimensions provide added conceptual value for
understanding the forms that moral injury may take in LGBTQ+ populations and
offer a framework for assessing identity-salient moral suffering that existing
instruments do not adequately capture (Nicholson et al., 2025; Ren et al.,
2018).
Validating this scale provides a critical tool for
early detection of severe moral distress among LGBTQ individuals, informing
culturally competent mental health practices and affirming therapeutic
interventions. Recent clinical frameworks emphasize that treatment of moral
injury requires addressing moral emotions, identity reconciliation, and
spiritual healing, over and above standard trauma-informed approaches (Griffin
et al., 2019). For LGBTQ persons in particular, affirmative therapy and
integration of spiritual resilience emerge as essential components to
counteract accumulated moral injury (Nicholson et al., 2025). Furthermore,
considering intersectional identities—such as race, ethnicity, socio-economic
status, and disability—is vital, as these factors influence the nature and
severity of moral injury experiences within subgroups of the LGBTQ population
(Nicholson et al., 2025). An instrument with validated psychometric properties
sensitive to these complex experiences supports nuanced research and equitable
clinical care.
To further situate the LGBT Moral Injury Scale within
established clinical constructs and to provide external validity evidence, the
present study also examines convergent validity with (a) posttraumatic stress
symptoms and (b) negative religious coping. Specifically, the PTSD Checklist
for DSM-5 (PCL-5) is a 20-item self-report instrument aligned with DSM-5
criteria that assesses PTSD symptom severity over the past month and has
demonstrated strong psychometric properties across diverse samples (Blevins et
al., 2015; Weathers et al., 2013). In parallel, the Negative Religious Coping
subscale of the Brief RCOPE captures religious responses marked by struggle
with the sacred—e.g., perceived divine punishment or abandonment and conflict
with one’s faith community—and is consistently associated with poorer
psychological outcomes (Pargament et al., 1998). Given the centrality of shame,
self-condemnation, and religious struggle in LGBTQ moral injury, we anticipate
that the LGBT-MIS will correlate positively with both PTSD severity and
negative religious coping, thereby providing theoretically coherent convergent
evidence.
In sum, this study advances the scientific
understanding of moral injury in LGBTQ individuals by providing an empirically
grounded, multidimensional assessment tool. This effort responds to a critical
gap in mental health research and practice, offering pathways to enhanced
detection, culturally attuned intervention, and, improved emotional and social
well-being for sexual and gender minorities (Bohren et al., 2022).
METHODS
Design
This study is framed within an instrumental design,
according to the classification proposed by Ato et al. (2013). Instrumental
research primarily aims to construct, adapt, and validate measurement
instruments, such as the LGBT Moral Injury Scale. This type of design is ideal
for examining the psychometric properties of an instrument, such as
reliability, validity, and factor structure. It provides evidence of its
adequacy for measuring the construct of interest in a specific population. The
instrumental design is characterized by a quantitative, cross-sectional, and
non-experimental approach, focused on collecting data at a single point in time
to evaluate how the proposed items and dimensions conform to and reflect the
theoretical construct under study (Ato et al., 2013). Moreover, this design
allows for performing exploratory and confirmatory
factor analyses, as well as tests of internal consistency and convergent and
discriminant validity.
Participants
We recruited participants through a paid social-media
advertisement (e.g., Facebook). Recruitment followed a non-probability
convenience approach, amplified via snowball sampling of the post. Surveys were
completed online in Spanish. To be eligible, respondents had to self-identify
as LGBT+, be 21 years or older, and reside in Puerto Rico. A total of 242
adults completed the sociodemographic questionnaire, with no missing data. Ages
ranged from 21 to 71 years (M = 39.55, SD = 13.89).
The final analytic sample of 242 participants was
considered adequate for an initial confirmatory factor analysis (CFA).
Methodological literature has noted that sample-size requirements in factor
analytic research depend on multiple model features, including the number of
factors, the number of items per factor, the magnitude of factor loadings,
correlations between factors, and overall model complexity (Knekta
et al., 2019; Wolf et al., 2013). In addition, although samples of around 200
participants are often regarded as acceptable starting points for initial CFA
applications, more recent work has emphasized that adequacy should be evaluated
in relation to model characteristics rather than relying exclusively on fixed
rules of thumb (Knekta et al., 2019; Wolf et al.,
2013). In the present study, the sample size was deemed sufficient for the
initial evaluation of the proposed models, particularly for the final 15-item,
five-factor solution. Nevertheless, given the use of non-probability sampling
and the preliminary nature of this validation study, the findings should be
interpreted cautiously and replicated in independent samples.
Most respondents identified their gender as male
(57.0%) or female (37.2%), with smaller groups identifying as transgender
(2.5%), non-binary (2.1%), or other (1.2%). For sex, 57.4% reported male, 41.3%
female, 0.4% intersex, and 0.8% other. Regarding sexual orientation, 51.2%
identified as gay, 22.7% as lesbian, 16.9% as bisexual, 5.8% as pansexual, and
3.3% as other. Relationship circumstances were diverse: single (45.0%),
partnered and cohabiting (24.0%), partnered and not cohabiting (12.8%), married
(14.0%), divorced (2.1%), separated (0.8%), and widowed (1.2%). Approximate
annual household income clustered at the lower brackets—$0–$20,000 (37.2%) and
$21,000–$30,000 (25.2%)—with fewer reporting $31,000–$40,000 (15.3%),
$41,000–$50,000 (6.6%), $51,000–$60,000 (5.0%), or $61,000 or more (10.7%).
Religious and spiritual identities were varied: spiritual but not religious
(28.1%), Catholic (27.7%), Protestant traditions (e.g., Evangelical, Methodist,
Baptist, Pentecostal; 16.5%), none (10.3%), agnostic (7.0%), atheist (4.5%),
Santería (2.1%), Buddhism (1.7%), Orthodox Christian (0.8%), and Adventist
(0.4%). Reported attendance at religious services was predominantly never
(55.8%), followed by once per year (21.5%), weekly (12.8%), monthly (9.1%), and
daily (0.8%). As for the perceived influence of religious beliefs on lifestyle,
33.9% described it as positive, 2.9% as negative, 36.0% reported no influence,
and 27.3% responded “maybe”.
Instruments
LGBT Moral Injury Scale (Spanish version; LGBT-MIS). The LGBT-MIS is a self-report measure developed by the principal
investigator and grounded in contemporary definitions and core dimensions of
moral injury (guilt/shame and concealment, sexual–moral dissonance,
spiritual/religious struggle, and global self-devaluation). The preliminary
instrument contains 30 items administered online in Spanish; each rated on a
6-point Likert scale (1 = Strongly disagree to 6 = Strongly agree). Higher
scores indicate greater moral injury.
Item development followed a theory-driven approach.
The principal investigator generated an initial pool of 35 items based on a
targeted review of the literature on moral injury, minority stress,
internalized stigma, shame, guilt, religious/spiritual struggle, and
identity-related conflict in LGBTQ+ populations. The goal of this stage was to
ensure conceptual coverage of the main dimensions theorized to characterize
moral injury in sexual and gender minorities. The preliminary item pool was
organized to reflect five provisional domains: guilt, shame, moral conflicts,
religious struggle, and self-condemnation.
After the initial drafting stage, content validity was
evaluated by eight expert judges using the Lawshe content validity method. All
eight judges held doctoral degrees, and their areas of expertise included
clinical psychology, psychometrics, LGBTQ+ mental health, and trauma. Judges
met two a priori criteria: (a) at least one professional publication in LGBT
studies and (b) basic training in psychometrics. Of the eight judges, three had
prior experience in research and instrument and scale development, whereas five
had extensive clinical, academic, and research experience focused on LGBTQ+
populations. This multidisciplinary composition was intended to strengthen both
the conceptual relevance and methodological rigor of the content-validation
process. For each item, we computed the Content Validity Ratio (CVR) and
applied the critical values recalculated by Wilson et al. (2012); for k = 8
judges, the acceptance threshold was CVR ≥ .693 (two-tailed α =
.05). Five items fell below this threshold and were removed, yielding the
30-item preliminary version used in subsequent psychometric analyses.
Posttraumatic Stress Disorder Checklist for DSM-5
(PCL-5). The PCL-5 is a 20-item self-report
measure aligned with DSM-5 criteria for posttraumatic stress disorder that
indexes symptom severity over the past month on a 5-point scale (0 = not at all
to 4 = extremely), yielding total scores from 0 to 80; higher scores reflect
greater PTSD severity (Blevins et al., 2015; Weathers et al., 2013). Following
common practice, we computed a total severity score. In the present sample, the
PCL-5 demonstrated strong internal consistency (α = .97; ω = .97).
Negative Religious Coping (Brief RCOPE-N). For convergent validity purposes, we administered only the
Negative Religious Coping subscale of the Brief RCOPE (7 items), which
captures struggle-oriented responses (e.g., perceived divine punishment or
abandonment; conflict within one’s faith community) in the context of stress
(Pargament, Smith, Koenig, & Perez, 1998). Items were rated on a scale from
1 (not at all) to 4 (a great deal). In this study, scoring was performed
by summing the seven items to yield a total Negative Religious Coping
score (range = 7–28), with higher values indicating greater negative religious
coping. A Spanish version with conceptual equivalence was administered. In the
present sample, the subscale showed satisfactory reliability (α = .88;
ω = .89).
Data Analysis
Data were analyzed using IBM SPSS Statistics (Version
30), Stata (Version 18), and Gaskin’s Stats Tools Package (Gaskin, 2016). We
screened item distributions (means, standard deviations, skewness, and
kurtosis). We assessed univariate normality with the Kolmogorov–Smirnov and
Shapiro–Wilk tests, and multivariate normality with the Doornik–Hansen, Mardia, and Henze–Zirkler tests
(Doornik & Hansen, 2008). Item quality was examined using corrected
biserial item–total correlations, indicator reliabilities (R²), and alpha if
deleted. Internal consistency for each factor was estimated using Cronbach’s
α and McDonald’s ω; values ≥ .70 were considered adequate
(DeVellis, 2017).
Given the LGBT-MIS’s 6-point Likert response format,
the CFA models were estimated using maximum likelihood with Satorra–Bentler
corrections to obtain robust standard errors and fit indices under
non-normality. Although the item responses were ordinal, simulation studies
have shown that variables with five or more ordered response categories can
often be treated as approximately continuous in SEM/CFA, particularly when the
goal is to obtain robust model-based estimates and compare competing models (Rhemtulla et al., 2012). Moreover, evidence comparing
robust maximum likelihood and ordinal estimators indicates that, although
categorical estimators may be preferable in many ordinal-data settings, robust
maximum likelihood can perform adequately under several practical conditions,
including models with six response categories and moderate sample sizes (Li,
2016). Accordingly, in this initial validation study, robust maximum likelihood
was used as a pragmatic approach to model estimation, given the clear lack of univariate
and multivariate normality. Model adequacy was judged holistically using the
SB-corrected χ², CFI, TLI, RMSEA, SRMR, and Akaike’s Information Criterion
(AIC) for model comparison, with lower AIC values indicating better expected
out-of-sample fit. We considered commonly cited guidelines (e.g., CFI/TLI
≥ .95; RMSEA ≤ .06–.08; SRMR ≤ .08; Byrne, 2010) together
with theoretical interpretability and parameter reasonableness; for competing
specifications, we also interpreted ΔAIC (e.g., differences ≥ 2 as
meaningful; Burnham & Anderson, 2002).
To evaluate convergent and discriminant validity of
the LGBT-MIS latent factors, we computed the Average Variance Extracted (AVE)
and, for discriminant evidence, the Maximum Shared Variance (MSV) and Average
Shared Variance (ASV) (Hair et al., 2019); these indices were obtained with the
Stats Tools Package (Gaskin, 2016). In addition, we incorporated two external
criteria to examine convergent validity. For the PTSD Checklist for DSM-5
(PCL-5), we computed a total severity score (0–80). For the Brief RCOPE—Negative
Religious Coping (Brief RCOPE-N), we administered only the 7 negative-coping
items and derived a sum score (range = 7–28), with higher scores indicating
greater negative religious coping. We estimated internal consistency (α
and ω) for both external measures in the present sample.
We then conducted Pearson correlations between
LGBT-MIS total and subscale scores and (a) PCL-5 total and (b) Brief RCOPE-N
(sum) to test convergent validity hypotheses. For all correlations, we reported
95% confidence intervals based on Fisher’s r-to-z transformation and
interpreted magnitudes using Champion’s scale (Champion, 1981): 0.00–0.25 =
low, 0.26–0.50 = moderately low, 0.51–0.75 = moderately high, and 0.76–1.00 =
high. The significance level was set at p < .05 (95% confidence) for all
inferential tests.
Ethical aspects
The protocol was reviewed and approved by the
Institutional Review Board (IRB) of Ponce Health Sciences University (PHSU),
Ponce, Puerto Rico. All participants provided written informed consent. Our
study was conducted in accordance with the Declaration of Helsinki.
RESULTS
Univariate and Multivariate Normality
At the item level, LGBT-MIS responses showed clear
departures from normality. Skewness was mostly positive, ranging from
−0.511 (Item 26) to 3.350 (Item 14), indicating concentration of
responses toward the lower end of the 6-point scale for many items. Kurtosis
ranged from −1.567 (Item 10) to 12.047 (Item 14), with several items
exhibiting pronounced leptokurtosis (e.g., Item 14: skew = 3.350, kurtosis =
12.047; Item 20: kurtosis = 8.786; Item 21: kurtosis = 5.907; Item 19: kurtosis
= 5.683). Formal tests converged on non-normality at the univariate level:
Kolmogorov–Smirnov statistics ranged D = .176–.465, and Shapiro–Wilk
coefficients ranged W = .442–.857 (all p < .001; see Table 1).
Table 1. Descriptive Statistics,
Normality, Item Quality Indices and Confidence Intervals for Factor Loadings
|
Item |
M |
SD |
Skew |
Kurt |
KS |
SW |
rbis |
R2 |
αid |
|
1 |
2.44 |
1.71 |
0.83 |
-0.69 |
0.27 |
0.79 |
0.70 |
0.69 |
0.93 |
|
2 |
1.92 |
1.39 |
1.48 |
1.16 |
0.33 |
0.70 |
0.72 |
0.68 |
0.93 |
|
3 |
1.81 |
1.35 |
1.72 |
1.96 |
0.36 |
0.65 |
0.76 |
0.77 |
0.93 |
|
4 |
1.71 |
1.33 |
1.95 |
2.77 |
0.40 |
0.59 |
0.75 |
0.73 |
0.93 |
|
5 |
1.92 |
1.50 |
1.54 |
1.16 |
0.37 |
0.66 |
0.71 |
0.65 |
0.93 |
|
6 |
2.32 |
1.72 |
1.02 |
-0.40 |
0.29 |
0.75 |
0.68 |
0.67 |
0.93 |
|
7 |
2.62 |
1.63 |
0.60 |
-0.94 |
0.22 |
0.85 |
0.64 |
0.63 |
0.93 |
|
8 |
1.81 |
1.28 |
1.51 |
1.23 |
0.37 |
0.67 |
0.76 |
0.69 |
0.93 |
|
9 |
1.63 |
1.27 |
2.28 |
4.52 |
0.41 |
0.56 |
0.57 |
0.48 |
0.93 |
|
10 |
3.48 |
1.95 |
-0.02 |
-1.57 |
0.18 |
0.85 |
-0.03 |
0.17 |
0.94 |
|
11 |
2.44 |
1.90 |
1.04 |
-0.51 |
0.29 |
0.72 |
0.07 |
0.20 |
0.94 |
|
12 |
2.65 |
1.71 |
0.63 |
-0.95 |
0.22 |
0.84 |
0.54 |
0.53 |
0.93 |
|
13 |
2.52 |
1.79 |
0.78 |
-0.89 |
0.26 |
0.79 |
0.49 |
0.40 |
0.93 |
|
14 |
1.36 |
0.92 |
3.35 |
12.05 |
0.46 |
0.44 |
0.45 |
0.45 |
0.93 |
|
15 |
1.52 |
1.16 |
2.56 |
6.07 |
0.44 |
0.51 |
0.62 |
0.59 |
0.93 |
|
16 |
2.24 |
1.65 |
1.10 |
-0.12 |
0.30 |
0.75 |
0.58 |
0.55 |
0.93 |
|
17 |
1.57 |
1.28 |
2.38 |
4.72 |
0.45 |
0.51 |
0.52 |
0.50 |
0.93 |
|
18 |
1.72 |
1.40 |
1.99 |
2.80 |
0.41 |
0.58 |
0.54 |
0.59 |
0.93 |
|
19 |
1.49 |
1.18 |
2.56 |
5.68 |
0.46 |
0.48 |
0.69 |
0.72 |
0.93 |
|
20 |
1.41 |
1.06 |
3.01 |
8.79 |
0.47 |
0.45 |
0.70 |
0.76 |
0.93 |
|
21 |
1.49 |
1.18 |
2.59 |
5.91 |
0.46 |
0.48 |
0.66 |
0.78 |
0.93 |
|
22 |
1.75 |
1.43 |
1.85 |
2.13 |
0.42 |
0.59 |
0.51 |
0.57 |
0.93 |
|
23 |
2.17 |
1.72 |
1.20 |
-0.06 |
0.36 |
0.69 |
0.34 |
0.35 |
0.93 |
|
24 |
2.19 |
1.75 |
1.17 |
-0.20 |
0.35 |
0.69 |
0.42 |
0.43 |
0.93 |
|
25 |
1.61 |
1.37 |
2.36 |
4.39 |
0.44 |
0.50 |
0.65 |
0.62 |
0.93 |
|
26 |
2.33 |
1.71 |
0.95 |
-0.51 |
0.31 |
0.76 |
0.62 |
0.81 |
0.93 |
|
27 |
2.17 |
1.66 |
1.17 |
-0.07 |
0.34 |
0.72 |
0.64 |
0.87 |
0.93 |
|
28 |
1.98 |
1.53 |
1.39 |
0.60 |
0.36 |
0.68 |
0.61 |
0.80 |
0.93 |
|
29 |
2.07 |
1.62 |
1.30 |
0.31 |
0.36 |
0.69 |
0.64 |
0.75 |
0.93 |
|
30 |
2.70 |
2.04 |
0.66 |
-1.28 |
0.30 |
0.75 |
0.55 |
0.58 |
0.93 |
Note: M = Mean; SD = Standard
deviation; Skew = Skewness; Kurt = Kurtosis; Standard error of skewness = .156;
Standard error of kurtosis = .312. KS = Kolmogorov-Smirnov; SW = Shapiro-Wilk;
Kolmogorov-Smirnov and Shapiro-Wilk degrees of freedom = 242, all p-values
< .001; rbis = discrimination indices; R2 = explained
variance; αid = Cronbach’s alpha if item deleted.
Multivariate normality was likewise rejected by
omnibus tests: Mardia’s skewness = 382.89, χ²(4,960) = 15,647.24, p < .001; Mardia’s
kurtosis = 1,385.67, χ²(1) = 5,709.44, p <
.001; Henze–Zirkler = 2.08, χ²(1)
= 7.45, p < .001; Doornik–Hansen χ²(60) =
3,552.73, p < .001. Given the lack of evidence for multivariate normality,
CFA models were estimated using robust maximum likelihood with Satorra–Bentler corrections (Satorra
& Bentler, 2001).
Confirmatory Factor Analysis
We tested five CFA specifications. M0 was a baseline
unidimensional model and, as expected, did not provide an adequate
representation of the data (see Table 2). M1 reflected the theoretical
five-factor structure of the LGBT-MIS and yielded a substantial improvement in
global fit relative to M0. We then explored three refinements. M2 retained the
four highest-loading items per factor (20 items total), showing additional
improvement. M3 removed the lowest-loading indicators observed in the
theoretical model, resulting in an 18-item solution with better fit and
parsimony. Finally, M4 retained three items per factor (15 items), prioritizing
content coverage, conceptual balance across the five theoretical dimensions,
and simplicity; this specification achieved the best overall fit among the
candidate models and the lowest AIC, thus becoming the selected solution (Table
2).
Table 2. CFA Model Fit Indices.
|
Model |
χ2sb |
DF |
RMSEAsb |
CFIsb |
TLIsb |
SRMR |
AIC |
|
M0 |
1,503.78 |
405 |
0.11 |
0.66 |
0.64 |
0.09 |
23,450.0 |
|
M1 |
736.22 |
395 |
0.06 |
0.90 |
0.88 |
0.06 |
22,406.4 |
|
M2 |
287.3 |
160 |
0.06 |
0.94 |
0.93 |
0.06 |
13,978.9 |
|
M3 |
204.13 |
125 |
0.05 |
0.96 |
0.95 |
0.05 |
12,413.4 |
|
M4 |
135.76 |
80 |
0.05 |
0.96 |
0.95 |
0.04 |
10,455.2 |
Note. M0 = baseline unidimensional
model; M1 = theoretical model; M4 = final model; df
= degrees of freedom; RMSEA = Root Mean Square Error of Approximation; CFI
= Comparative Fit Index; TLI = Tucker–Lewis Index; SRMR =
Standardized Root Mean Square Residual; AIC = Akaike Information
Criterion; SB = Satorra–Bentler correction. All
χ² statistics were significant (p < .001).
Item reduction was guided by both statistical and
conceptual criteria rather than by fixed loading cutoffs alone. From a
statistical standpoint, we prioritized indicators with stronger standardized
loadings, adequate corrected item discrimination, and better contribution to
global model fit and parsimony across competing CFA solutions. From a
conceptual standpoint, we sought to preserve the theoretical breadth of each
proposed domain so that the final version would retain meaningful coverage of
guilt, shame, moral conflicts, religious struggle, and self-condemnation.
Accordingly, items were not removed solely because of relatively lower
loadings; retention decisions also considered whether an item represented a
conceptually important aspect of the latent dimension. The final M4 solution
retained three indicators per factor, balancing psychometric adequacy,
conceptual interpretability, and practical brevity.
Consistent with guidance that treats loading
thresholds as heuristic rather than rigid, retaining indicators with
standardized loadings ≥ .62 is supported by classic and contemporary
benchmarks (e.g., ≈ .60 classified as good and ≥ .63 as very good;
Comrey & Lee, 1992), as well as by SEM texts that accept loadings ≥
.50 as adequate for reflective indicators when the factor shows satisfactory
reliability and the model exhibits strong global fit and parsimony (Brown,
2015; Hair et al., 2019; Kline, 2016). Figure 1 displays the final model (M4)
for the LGBT-MIS.
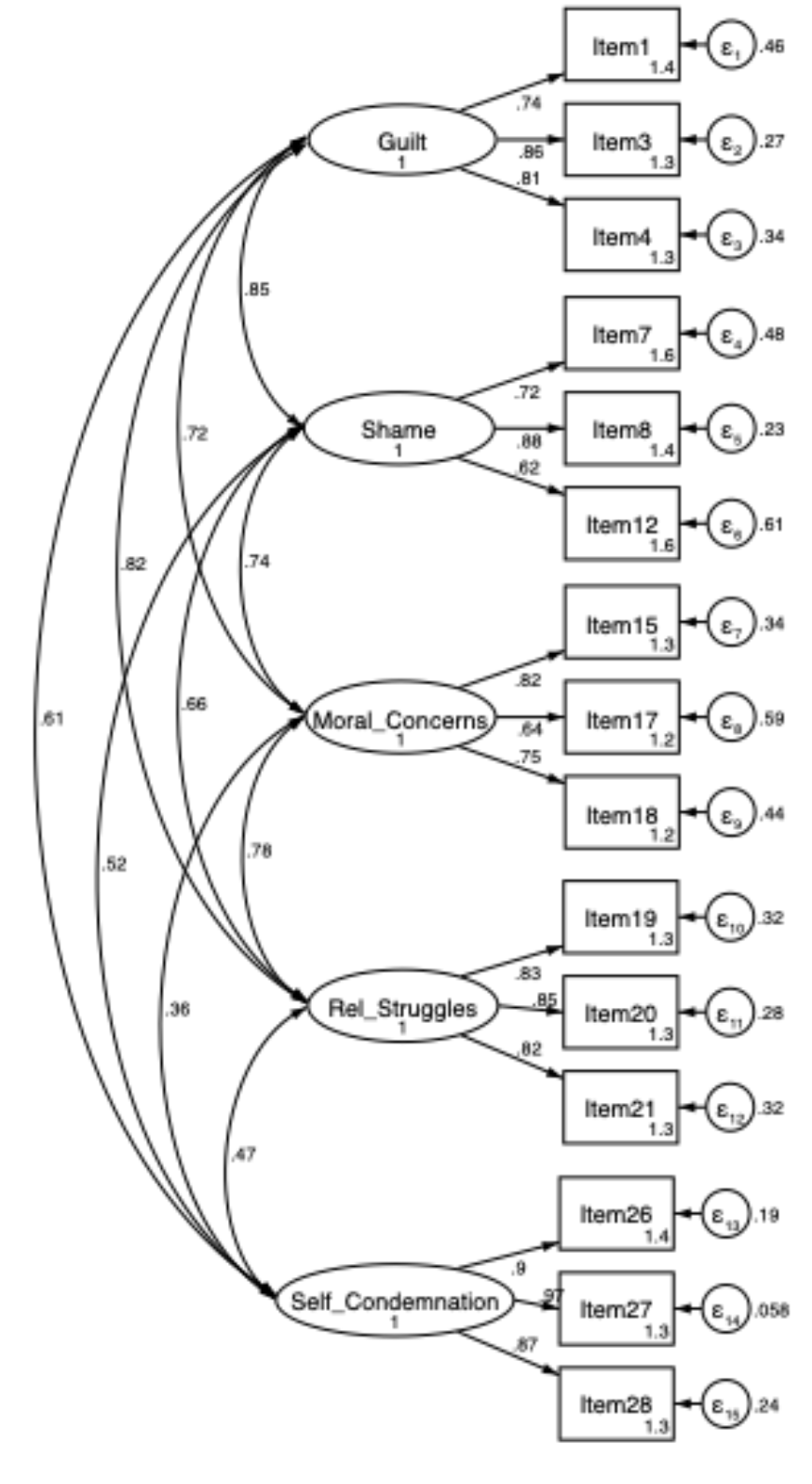
Figure 1. CFA of the final model (M4) of the LGBT Moral Injury Scale.
Internal Consistency and Item Discrimination
Item discrimination for each M4 factor was examined
using the corrected biserial discrimination index (rbisc)
/ corrected item–total correlation. All items within each M4 factor showed
adequate discrimination, with all values > .30 (see Table 3). Internal
consistency for the M4 factors was estimated using Cronbach’s alpha, McDonald’s
omega, and composite reliability. Findings indicated that each M4 factor
achieved adequate reliability, with α and ω > .70 (see Table 3).
Table 3. Discrimination Indices,
Standardized Regression Coefficient, and Confidence Intervals.
|
|
Items |
rbisc |
β |
95% CIsb |
|
1 |
I feel guilty for failing my
family’s expectations [Me
siento culpable por no cumplir con las expectativas de mi familia]. |
0.670 |
0.735 |
[.671, .799] |
|
3 |
I feel guilty for not being
heterosexual or cisgender [Me siento culpable por no ser heterosexual o cisgénero]. |
0.750 |
0.855 |
[.798, .913] |
|
4 |
I feel guilty for being who
I am [Me siento culpable por
ser quien soy]. |
0.690 |
0.810 |
[.740, .879] |
|
7 |
If people knew about my sexual orientation or gender identity, they would think
less of me than they do now [Si las personas supieran mi orientación sexual o
identidad de género, tendrían una opinión más negativa de mí que la que
tienen ahora]. |
0.670 |
0.721 |
[.647, .794] |
|
8 |
I feel ashamed of my sexual orientation or gender identity [Siento
vergüenza de mi orientación sexual o identidad de género]. |
0.640 |
0.877 |
[.821, .932] |
|
12 |
I feel embarrassed to speak in public
about my sexual orientation or gender identity [Me
avergüenza hablar en público sobre mi orientación sexual o identidad de
género]. |
0.620 |
0.623 |
[.518, .727] |
|
15 |
Because of my principles, I would like to change
my sexual orientation
and/or gender identity [Por mis principios, desearía cambiar mi
orientación sexual y/o identidad de género]. |
0.670 |
0.815 |
[.721, .909] |
|
17 |
From
a moral point of view, being heterosexual and cisgender is morally right [Desde el
punto de vista moral, ser heterosexual y cisgénero es lo moralmente
correcto]. |
0.530 |
0.639 |
[.499, .779] |
|
18 |
I enjoy my sexuality, but I
recognize that it is not morally correct [Disfruto
mi sexualidad, pero reconozco que no es moralmente correcto]. |
0.580 |
0.737 |
[.641, .854] |
|
19 |
I wonder what I did for God
to punish me [Me pregunto qué
hice para que Dios me castigue]. |
0.730 |
0.826 |
[.746, .906] |
|
20 |
I feel that God punishes me for my sexual orientation and/or gender identity
[Siento que Dios me castiga por mi orientación sexual y/o identidad de
género]. |
0.750 |
0.847 |
[.760, .934] |
|
21 |
I wonder whether God has
abandoned me [Me pregunto si
Dios me ha abandonado]. |
0.790 |
0.824 |
[.745, .903] |
|
26 |
At times I feel useless [En
ocasiones, me siento inútil]. |
0.860 |
0.899 |
[.850, .947] |
|
27 |
At times I feel that I am
worthless [En ocasiones, siento
que no sirvo para nada]. |
0.910 |
0.970 |
[.937, .999] |
|
28 |
Overall, I tend to feel that
I am a failure [En general, me inclino a sentir que soy un fracaso]. |
0.820 |
0.871 |
[.826, .917] |
Note. rbisc = corrected biserial
discrimination index (corrected item–total correlation); β = standardized
regression coefficient for each item; CIsb
= confidence interval with the Satorra–Bentler
correction for non-normality.
Convergent Validity, Discriminant Validity, and Correlations
Convergent validity was evaluated using the AVE, with
AVE ≥ .50 indicating adequate convergence (Fornell & Larcker, 1981).
All five M4 factors met this criterion, indicating that the retained items
adequately represented their intended constructs. Discriminant validity was
examined using the MSV and ASV, with evidence supported when both MSV and ASV
are lower than the AVE (Hair et al., 2019). By this standard, all factors met
the ASV criterion; however, Guilt, Shame, and Moral Conflicts did not fully
meet the stricter MSV < AVE criteria, indicating partial overlap among these
three dimensions (see Table 4). Given the close conceptual relatedness of these
constructs, some shared variance was expected. Taken together with the strong
global fit of the final model, the salience of the retained loadings, and the
absence of problematic cross-loadings, these findings support adequate
convergent validity for all factors and overall acceptable, although somewhat
limited, discriminant validity among these three conceptually adjacent
constructs. Finally, pairwise relationships among the five M4 factors were
positive and statistically significant, ranging from moderately low to
moderately high (see Table 4).
Table 4. Descriptive Statistics,
Internal Consistency, Convergent Validity, Discriminant Validity, and
Correlations.
|
Factor |
M |
SD |
α |
ω |
CR |
AVE |
MSV |
ASV |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
|
1. Guilt |
5.96 |
3.82 |
0.83 |
0.83 |
0.85 |
0.65 |
0.73nc |
0.57 |
— |
||||||
|
2. Shame |
7.07 |
3.91 |
0.79 |
0.80 |
0.79 |
0.56 |
0.73nc |
0.49 |
0.66 |
— |
|||||
|
3. Moral
Conflicts |
4.83 |
3.18 |
0.76 |
0.76 |
0.78 |
0.55 |
0.61nc |
0.45 |
0.56 |
0.55 |
— |
||||
|
4.
Religious Struggle |
4.39 |
3.05 |
0.87 |
0.87 |
0.87 |
0.70 |
0.68 |
0.48 |
0.68 |
0.51 |
0.65 |
— |
|||
|
5. Self-Condemnation |
6.51 |
4.63 |
0.93 |
0.94 |
0.94 |
0.84 |
0.37 |
0.25 |
0.56 |
0.42 |
0.32 |
0.43 |
— |
||
|
6. PCL-5 Total |
22.65 |
20.39 |
0.97 |
0.97 |
- |
- |
- |
0.47 |
0.35 |
0.31 |
0.46 |
0.57 |
— |
||
|
7. Brief RCOPE-N |
9.54 |
4.30 |
0.88 |
0.89 |
- |
- |
- |
0.41 |
0.35 |
0.38 |
0.57 |
0.30 |
0.34 |
— |
|
|
8.
LGBT-MIS Total |
37.09 |
19.70 |
0.92 |
0.91 |
|
- |
- |
- |
0.88 |
0.78 |
0.75 |
0.80 |
0.73 |
0.57 |
0.51 |
Note. M = mean; SD = standard
deviation. α = Cronbach’s alpha; ω = McDonald’s omega; CR = composite
reliability; AVE = Average Variance Extracted; MSV = Maximum Shared Variance;
ASV = Average Shared Variance; nc = does
not meet criteria). All correlations were significant at p < .001.
External convergent validity with PTSD symptoms and negative religious
coping
Consistent with predictions, the LGBT-MIS total score
correlated positively with PTSD severity (PCL-5) and with Negative Religious
Coping (Brief RCOPE-N), showing moderately high and moderately low magnitudes,
respectively, according to Champion’s scale. At the subscale level,
associations with PCL-5 were most pronounced for Self-Condemnation, followed by
Guilt, with Religious Struggle and Shame showing moderate associations and
Moral Conflicts, the smallest positive association. For Brief RCOPE-N, the strongest
association was observed for Religious Struggle, followed by Self-Condemnation,
with Guilt and Moral Conflicts in the mid-range and Shame showing the smallest
positive association. All effects were significant at p < .001 (see Table
4).
DISCUSSION
This study introduces the LGBT Moral Injury Scale
(LGBT-MIS) and provides initial and preliminary psychometric support for a
multidimensional assessment of moral injury tailored to LGBTQ+ populations.
Consistent with contemporary conceptualizations of moral injury as a syndrome
characterized by guilt, shame, moral disorientation, and self-condemnation
(Griffin et al., 2019; Litz et al., 2009), the final 15-item solution (M4)
demonstrated adequate fit under robust estimation, good internal consistency, satisfactory
item discrimination, and convergent validity. These findings extend literature
historically centered on military personnel (Koenig et al., 2019; Maguen et al., 2022) by operationalizing morally injurious
processes embedded in minority-stress contexts among SGM (Bohren et al., 2022;
Meyer, 2003; Nicholson et al., 2025).
The retained five-factor structure—Guilt, Shame, Moral
Conflicts, Religious Struggle, and Self-Condemnation—maps closely onto
theorized components of moral injury (Griffin et al., 2019; Litz et al., 2009;
Litz et al., 2022). Guilt captured perceived failure to meet familial and
societal expectations tied to sexual or gender identity; Shame reflected
anticipated negative evaluation and concealment; Moral Conflicts indexed
dissonance between personal values and hetero/cisnormative
moral codes; Religious Struggle encompassed perceived divine punishment,
abandonment, and the need for forgiveness; and Self-Condemnation represented
global negative self-evaluation and diminished self-respect.
The moderate positive intercorrelations among factors,
alongside mixed discriminant-validity evidence based on MSV (with ASV
supportive), point to a common moral-injury core with distinguishable—but
closely related—facets. This pattern mirrors prior work showing that shame and
guilt are intertwined yet separable moral emotions (Tangney & Dearing,
2002) and that moral-injury measures frequently exhibit correlated (and
sometimes bifactor) structures (Currier et al., 2020; Tappenden et al., 2024).
Within a minority-stress framework, concealment, anticipated rejection, and
internalized stigma create identity-salient PMIEs that activate these emotions
and value conflicts in LGBTQ+ persons (Bohren et al., 2022; Meyer, 2003;
Nicholson et al., 2025). Practically, this implies that subscale scores can
highlight predominant areas of distress (e.g., religious struggle vs.
self-condemnation), while an overall score indexes global moral-injury
severity.
The partial overlap observed among Guilt, Shame, and
Moral Conflicts warrants particular attention. Although these dimensions were
retained as distinct facets of the LGBT-MIS, their empirical proximity is
theoretically understandable within LGBTQ+ populations. Experiences of minority
stress often involve simultaneous exposure to rejection, concealment,
internalized stigma, and conflict with heteronormative or cisnormative
social expectations. In such contexts, individuals may not only experience
shame in response to anticipated or actual negative evaluation but also guilt
related to perceived failure to meet familial, cultural, or religious
expectations, alongside broader moral conflict regarding the compatibility of
their identity with dominant value systems. Thus, some degree of shared
variance among these factors is expected and may reflect the interwoven nature
of identity-related moral suffering rather than a failure of the construct. At
the same time, their partial overlap suggests that future research should
continue examining their factorial boundaries using complementary approaches,
such as HTMT and higher-order or bifactor models.
Beyond internal structure, the observed pattern of
external convergent validity situates the LGBT-MIS within clinically salient
networks. The total score showed the expected positive associations with PTSD
symptom severity and with Negative Religious Coping, supporting linkage to
trauma-related emotional processes and spiritually framed struggles. At the
facet level, the strongest link with PTSD was observed for Self-Condemnation,
aligning with models in which self-directed moral emotions and global negative
self-appraisals reinforce avoidance, hyperarousal, and negative alterations in
cognition and mood (Litz et al., 2009; Griffin et al., 2019; Litz et al.,
2022). The most proximal association with Negative Religious Coping emerged for
Religious Struggle, consistent with accounts that position spiritually oriented
struggle—e.g., perceptions of divine punishment/abandonment or conflict with
faith communities—as a mechanism that can intensify moral disorientation and
impede meaning-making in LGBTQ+ contexts (see Currier et al., 2019; Exline et
al., 2014; Park et al., 2023). Taken together, these convergences reinforce a
view of moral injury as embedded in both trauma phenomenology and spiritual
struggle, especially where minority-stress processes heighten vulnerability.
Although the associations with PTSD symptoms and Negative Religious Coping
provide theoretically coherent external support for the LGBT-MIS, they should
be interpreted as initial convergent evidence rather than as a comprehensive
test of the broader nomological network of LGBTQ+-related moral injury.
The prominence of Religious Struggle in this Puerto
Rican sample is theoretically meaningful. In Puerto Rico, questions of
sexuality and gender identity often unfold within a broader sociocultural
context shaped by religious traditions, family expectations, and community
norms. Even when individuals do not actively participate in organized religion,
religiously informed beliefs and moral discourses may remain influential in
shaping how sexual and gender diversity is interpreted, judged, or
internalized. Thus, spiritual pain may persist outside formal religious
participation and may be expressed through feelings of divine punishment,
abandonment, moral conflict, or the perceived need for forgiveness. In the
present sample, this interpretation is consistent with the substantial
proportion of participants identifying as Catholic or spiritual but not
religious, despite relatively low religious-service attendance. This pattern
aligns with evidence linking religious and spiritual struggles to poorer
mental-health outcomes (Currier et al., 2019; Exline et al., 2014; Park et al.,
2023) and underscores the value of interventions that address faith-related
meaning-making alongside identity affirmation. The convergent pattern with
Negative Religious Coping further suggests that, when moral injury is entangled
with conflicted relationships to the sacred or to religious communities,
addressing spiritually framed cognitions and practices may be integral to moral
repair.
The LGBT-MIS advances moral-injury assessment in
several ways. First, it offers content-valid coverage of LGBTQ+-salient PMIEs
by integrating identity-related guilt/shame, moral dissonance with hetero-/cisnormative codes, and religious/spiritual struggle into
one instrument. Content validity was established a priori with a transparent
CVR decision rule (Wilson et al., 2012), ensuring that retained items were
judged essential by qualified experts. The subsequent CFA program with Satorra–Bentler corrections addressed observed
non-normality (Satorra & Bentler, 2001), and
selecting a parsimonious 15-item structure (three indicators per factor)
improved interpretability, maintained strong global fit, and minimized AIC
relative to the theoretical and unidimensional alternatives. This approach follows
contemporary guidance to balance psychometric evidence with conceptual coverage
rather than enforce rigid loading cutoffs (Brown, 2015; Hair et al., 2019;
Kline, 2016).
Second, the scale demonstrates a robust internal
structure and score reliability. All factors exceeded conventional thresholds
for internal consistency (α, ω ≥ .74), and item discrimination
statistics indicated that retained items contribute meaningfully to their
factors. In addition, composite reliability coefficients derived from the final
factor model were satisfactory across the five dimensions, ranging from .78 to
.94, thus providing further model-based evidence of score reliability.
Convergent validity was uniformly adequate (AVE ≥ .50), comparable to or
exceeding values reported for established moral-injury tools in non-military
samples (Bryan et al., 2016; Currier et al., 2020; Tappenden et al., 2024).
Although MSV > AVE for Guilt, Shame, and Moral Conflicts indicate overlap,
this is theoretically coherent given the shared moral-emotion core of the
construct (Griffin et al., 2019; Tangney & Dearing, 2002; Litz et al.,
2022). Future confirmatory work should explicitly test higher-order or bifactor
models to quantify the contribution of a general moral-injury factor while
preserving clinically informative subscales (Currier et al., 2020; Litz et al.,
2022; Tappenden et al., 2024). As a complementary sensitivity analysis,
evaluating HTMT may further clarify discriminant evidence.
Third, the LGBT-MIS is practice-ready for
Spanish-speaking contexts while remaining extensible for cross-cultural
research. Using item-mean scoring (1–6) facilitates interpretation and
communication of change over time in clinical and program-evaluation settings.
The measure fills a gap left by instruments developed primarily for military or
health-professional populations (Bryan et al., 2016; Currier et al., 2020;
Tappenden et al., 2024; Litz et al., 2022), and it does so with explicit
attention to identity-specific moral tensions highlighted by minority-stress
scholarship (Bohren et al., 2022; Meyer, 2003; Nicholson et al., 2025).
Next-step psychometric studies should examine measurement invariance (e.g., by
gender identity, sexual orientation, religious affiliation), differential item
functioning, and test–retest reliability; compare robust ML vs. ordinal
estimators; and apply IRT models for polytomous items to inform short forms and
adaptive testing.
Clinically, the LGBT-MIS enables a mechanism-focused
assessment that complements trauma-focused screening. The total score indexes
global moral-injury severity, while subscale profiles help tailor case
formulations: prominent Religious Struggle may call for spiritually integrated
care and meaning reconstruction (Currier et al., 2019; Exline et al., 2014;
Park et al., 2023); elevated Shame may prioritize compassion-based,
acceptance-focused, or exposure-with-compassion strategies; heightened Moral
Conflicts may benefit from values clarification and moral reasoning work; and
Self-Condemnation suggests targeting global self-evaluation and worth. The
external convergent findings further justify integrated assessment that
includes (a) routine screening for PTSD symptoms and (b) brief appraisal of
religious/spiritual struggle when elevated LGBT-MIS scores are observed. The
instrument supports treatment planning and monitoring, including integration
with Adaptive Disclosure and related MI-focused approaches adapted for LGBTQ+
clients (Litz et al., 2024; Griffin et al., 2019). Because moral injury is
linked to PTSD symptoms, depression, substance use, and suicidality (Griffin et
al., 2019; Koenig et al., 2019; Maguen et al., 2022),
higher scores—especially on Shame and Self-Condemnation—should trigger risk
assessment, stepped-care triage, and referral pathways within affirmative
practice frameworks.
For research, the LGBT-MIS offers a unified outcome
and mechanism measure to test models linking PMIE exposure, minority-stress
processes, religious/spiritual struggle, and mental-health outcomes (Bohren et
al., 2022; Meyer, 2003; Nicholson et al., 2025; Currier et al., 2019; Exline et
al., 2014; Park et al., 2023). The convergent pattern with PTSD and Negative
Religious Coping motivates longitudinal and mechanistic designs to evaluate
mediation and moderation—for example, whether changes in Shame or Self-Condemnation
mediate symptom improvement, or whether Religious Struggle or Negative
Religious Coping moderate the impact of PMIEs on distress. The LGBT-MIS can be
paired with syndrome-level indices such as the Moral Injury Outcome Scale
(MIOS) (Litz et al., 2022) to map how specific facets relate to global
impairment. Cross-cultural studies should develop language adaptations (e.g.,
English via back-translation) and establish norms and cut-points for diverse
LGBTQ+ subgroups. Finally, combining the LGBT-MIS with validated measures of
minority stress, stigma, and spirituality can clarify incremental validity and
inform multilevel interventions (e.g., clinician training, policy, and
partnerships with affirming faith communities) aimed at reducing morally injurious
contexts—not only their psychological sequelae (Bohren et al., 2022; Meyer,
2003; Nicholson et al., 2025; Litz et al., 2022).
Generalizability is limited by convenience sampling
within Puerto Rico and snowball recruitment. The cross-sectional, self-report
design raises concerns about shared method variance and social desirability.
Accordingly, the present findings should be interpreted as preliminary evidence
of validity rather than as definitive confirmation of the scale’s psychometric
properties. Although CFA supported the five-factor model after item reduction
to 15 indicators, we did not conduct cross-validation in an independent sample.
Discriminant validity was not fully supported by MSV for Guilt, Shame, and
Moral Conflicts, and we did not assess test–retest reliability, sensitivity to
change, or measurement invariance across key subgroups. Because the sample was
non-probabilistic and restricted to Puerto Rico, the extent to which the factor
structure generalizes to other LGBTQ+ populations and cultural contexts remains
to be established. In addition, the present external validation strategy was
limited to PTSD symptom severity and Negative Religious Coping; therefore,
broader validity evidence involving constructs such as minority stress,
internalized stigma, psychological well-being, and other moral injury measures remain
to be established.
Future work should: (1) cross-validate the 15-item
model and test higher-order/bifactor alternatives; (2) evaluate measurement
invariance across subgroups and languages (including an English adaptation) and
assess differential item functioning; (3) establish test–retest reliability,
clinical cut-points, and responsiveness to intervention; (4) broaden convergent
and incremental validity testing by examining associations with minority-stress
constructs, internalized stigma, psychological well-being, moral emotions, and
other moral injury measures, as well as predictive validity for clinical
outcomes; (5) apply IRT to refine items and information functions, enabling
short forms and computerized adaptive testing; and (6) develop normative data
and interpretive bands for diverse SGM populations.
The LGBT-MIS demonstrates promising structural
validity, reliability, and convergent validity as a measure of moral injury
tailored to LGBTQ adults. Its five interrelated facets capture guilt, shame,
moral dissonance, religious/spiritual struggle, and self-condemnation—core
experiences that extend the moral-injury construct beyond military contexts and
into the lived realities of sexual and gender minorities. With further
validation and cross-cultural testing, the LGBT-MIS can support earlier
detection, targeted intervention, and culturally attuned care, advancing both
research and practice aimed at reducing moral distress and improving the
well-being of LGBTQ communities. For ease of use in future research, the
complete final version of the LGBT-MIS, including administration instructions,
is presented in Appendix A.
ORCID
Juan
Aníbal González-Rivera: https://orcid.org/0000-0003-0622-8308
Adam Rosario-Rodríguez: https://orcid.org/0000-0003-1603-5040
AUTHORS’ CONTRIBUTION
Juan Aníbal
González-Rivera: Conceptualization, Investigation, Writing - Original Draft,
Writing - Review & Editing, Visualization, Project administration.
Adam
Rosario-Rodríguez: Methodology, Formal analysis, Writing - Original Draft,
Visualization.
FUNDING
SOURCE
This study was not funded by
any entity or sponsor.
CONFLICT
OF INTEREST
The authors declare that there were no
conflicts of interest in the collection of data, analysis of information, or
writing of the manuscript.
ACKNOWLEDGMENTS
Not applicable.
REVIEW
PROCESS
This study has been reviewed by Claudia Guevara Cordero and Fernando
Joel Rosario Quiroz in double-blind mode. The editor in charge was David Villarreal-Zegarra.
The review process is included as supplementary material 1.
DATA AVAILABILITY
STATEMENT
Researchers and
academics interested in accessing the research data may contact the
corresponding author via email.
DECLARATION OF THE USE OF GENERATIVE ARTIFICIAL INTELLIGENCE
The authors used DeepL
to translate specific sections of the manuscript and Grammarly to improve the
wording of certain sections.
DISCLAIMER
The authors are responsible for all statements made in this article.
REFERENCES
Ato, M., López‑García, J. J. L., & Benavente, A. (2013).
Un sistema de clasificación de los diseños de investigación en psicología [A
classification system for research designs in psychology]. Anales de Psicología, 29(3), 1038–1059. https://doi.org/10.6018/analesps.29.3.178511
Blevins, C. A., Weathers, F. W., Davis, M.
T., Witte, T. K., & Domino, J. L. (2015). The Posttraumatic Stress Disorder
Checklist for DSM-5 (PCL-5): Development and initial psychometric
evaluation. Journal of Traumatic Stress, 28(6), 489–498. https://doi.org/10.1002/jts.22059
Bohren, M. A., Vazquez Corona, M., Odiase,
O. J., Wilson, A. N., Sudhinaraset, M.,
Diamond-Smith, N., Berryman, J., Tunçalp, Ö., & Afulani, P. A. (2022). Strategies to reduce stigma and
discrimination in sexual and reproductive healthcare settings: A mixed‑methods
systematic review. PLOS Global Public Health, 2(7), e0000582. https://doi.org/10.1371/journal.pgph.0000582
Brown, T. A. (2015). Confirmatory factor
analysis for applied research (2nd ed.). Guilford Press.
Bryan, C. J., Bryan, A. O., Anestis, M.
D., Anestis, J. C., Green, B. A., Etienne, N., Morrow, C. E., & Ray-Sannerud, B. (2016). Measuring moral injury: Psychometric
properties of the Moral Injury Events Scale in two military samples. Assessment,
23(5), 557-570. https://doi.org/10.1177/1073191115590855
Burnham, K. P., & Anderson, D. R. (2002). Model
selection and multimodel inference: A practical
information-theoretic approach (2nd ed.). Springer.
Byrne, B. M. (2010). Structural equation modeling
with AMOS: Basic concepts, applications, and programming. Psychology Press.
Champion, D. J. (1981). Basic
statistics for social research (2nd ed.). MacMillan.
Comrey, A. L., & Lee, H. B. (1992). A
first course in factor analysis (2nd ed.). Lawrence Erlbaum.
Currier, J. M., Foster, J. D., Witvliet, C. V., Abernethy, A. D., Root Luna, L. M.,
Schnitker, S. A., VanHarn, K., & Carter, J. (2019). Spiritual struggles and
mental health outcomes in a spiritually integrated inpatient program. Journal
of Affective Disorders, 249, 127–135. https://doi.org/10.1016/j.jad.2019.02.012
Currier, J. M., Isaak, S. L., &
McDermott, R. C. (2020). Validation of the Expressions of Moral Injury
Scale—Military Version—Short Form. Clinical Psychology & Psychotherapy,
27(1), 61–68. https://doi.org/10.1002/cpp.2407
DeVellis, R. F. (2017). Scale development: Theory and applications (4th Ed). Sage
Publications.
Doornik, J. A., & Hansen, H. (2008).
An omnibus test for univariate and multivariate normality. Oxford Bulletin
of Economics and Statistics, 70(5), 927–939. https://doi.org/10.1111/j.1468-0084.2008.00537.x
Exline, J. J., Pargament, K. I., Grubbs,
J. B., & Yali, A. M. (2014). The Religious and Spiritual Struggles Scale:
Development and initial validation. Psychology of Religion and Spirituality,
6(3), 208–222. https://doi.org/10.1037/a0036465
Flora, D. B., & Curran, P. J. (2004).
An empirical evaluation of alternative methods of estimation for confirmatory
factor analysis with ordinal data. Psychological Methods, 9(4),
466–491. https://doi.org/10.1037/1082-989X.9.4.466
Fornell, C., & Larcker, D. F. (1981).
Evaluating structural equation models with unobservable variables and
measurement error. Journal of Marketing Research, 18(1), 39–50. https://doi.org/10.1177/002224378101800104
Gaskin, J. (2016). Stats tools package.
http://statwiki.gaskination.com (Retrieved September 11, 2025).
Griffin, B. J., Purcell, N., Burkman, K.,
Litz, B. T., Bryan, C. J., Schmitz, M., Villierme, C., Walsh, J., & Maguen, S. (2019). Moral injury: An integrative review. Journal
of Traumatic Stress. https://doi.org/10.1002/jts.22362
Hair, J. F., Black, W. C., Babin, B. J.,
& Anderson, R. E. (2019). Multivariate data analysis (8th ed.). Cengage.
Herek, G. M. (2007). Confronting sexual
stigma and prejudice: Theory and practice. Journal of Social Issues, 63(4),
905–925. https://doi.org/10.1111/j.1540-4560.2007.00544.x
Herron, P. D. (2020). Current perspectives
on the impact of pre‑exposure prophylaxis stigma regarding men who have
sex with men in the United States. HIV/AIDS (Auckland, N.Z.), 12,
187–192. https://doi.org/10.2147/HIV.S214380
Kline, R. B. (2016). Principles and
practice of structural equation modeling (4th ed.). Guilford Press.
Knekta, E., Runyon, C., & Eddy, S.
(2019). One Size Doesn't Fit All: Using Factor Analysis to Gather Validity
Evidence When Using Surveys in Your Research. CBE life sciences
education, 18(1), rm1. https://doi.org/10.1187/cbe.18-04-0064
Koenig, H., Youssef, N., & Pearce, M.
J. (2019). Assessment of moral injury in veterans and active
duty military personnel with PTSD: A review. Frontiers in Psychiatry,
10, 443. https://doi.org/10.3389/fpsyt.2019.00443
Li, C.-H. (2016). Confirmatory factor
analysis with ordinal data: Comparing robust maximum likelihood and diagonally
weighted least squares. Behavior Research Methods, 48(3), 936–949. https://doi.org/10.3758/s13428-015-0619-7
Litz, B. T., Lebois,
L., Silver, R. C., et al. (2022). Defining and assessing the syndrome of moral
injury and developing the Moral Injury Outcome Scale (MIOS). Frontiers in
Psychiatry, 13, 923928. https://doi.org/10.3389/fpsyt.2022.923928
Litz, B. T., Stein, N., Delaney, E.,
Lebowitz, L., Nash, W. P., Silva, C., & Maguen,
S. (2009). Moral injury and moral repair in war veterans: A preliminary model
and intervention strategy. Clinical Psychology Review, 29(8),
695–706. https://doi.org/10.1016/j.cpr.2009.07.003
Litz, B. T., Yeterian, J., Berke, D.,
Lang, A. J., Gray, M. J., Nienow, T., Frankfurt, S., Harris, J. I., Maguen, S., & Rusowicz-Orazem,
L. (2024). A controlled trial of adaptive disclosure–enhanced to
improve functioning and treat posttraumatic stress disorder. Journal of
Consulting and Clinical Psychology, 92(3), 150–164. https://doi.org/10.1037/ccp0000873
Maguen, S., Griffin, B. J., Vogt, D., Hoffmire,
C. A., Blosnich, J. R., Bernhard, P. A., Akhtar, F.
Z., Cypel, Y. S., & Schneiderman, A. I. (2022).
Moral injury and peri‑ and post‑military suicide attempts among
post‑9/11 veterans. Psychological Medicine, 52(8),
1491–1500. https://doi.org/10.1017/S0033291721005274
Mantri, S., Lawson, J., Wang, Z., &
Koenig, H. (2020). Identifying moral injury in healthcare professionals: The
Moral Injury Symptom Scale‑HP. Journal of Religion and Health, 59(6),
3051–3065. https://doi.org/10.1007/s10943-020-01065-w
Meyer, I. H. (2003). Prejudice, social
stress, and mental health in lesbian, gay, and bisexual populations: Conceptual
issues and research evidence. Psychological Bulletin, 129(5),
674–697. https://doi.org/10.1037/0033-2909.129.5.674
Nicholson, A. A., Narikuzhy,
S., Wolf, J., Pichtikova, M., Siegel, M., Mirabelli,
J., Hatchard, T., Hosseini-Kamkar, N., Bawagan, E.,
Roth, S. L., Mutschler, C., Lanius, R. A., Hosseiny,
F., Eckstrand, K., & Lueger-Schuster, B. (2025).
Identity in turmoil: Investigating the morally injurious dimensions of minority
stress. European Journal of Psychotraumatology,
16(1), 2479396. https://doi.org/10.1080/20008066.2025.2479396
Pargament, K. I., Smith, B. W., Koenig, H.
G., & Perez, L. (1998). Patterns of positive and negative religious coping
with major life stressors. Journal for the Scientific Study of
Religion, 37(4), 710–724. https://doi.org/10.2307/1388152
Park, C. L., Silverman, E. J., Sacco, S.
J., Kim, D., Hall, M. E. L., McMartin, J., Kapic, K., Shannonhouse, L., David,
A. B., & Aten, J. (2023). When suffering contradicts belief: Measuring theodical struggling. Current Psychology, 1–13. https://doi.org/10.1007/s12144-023-04642-w
Ren, Z., Howe, C. Q., & Zhang, W.
(2018). Maintaining mianzi and lizi:
Understanding the reasons for formality marriages between gay men and lesbians
in China. Sexual and Relationship Therapy, 33(5), 465–482. https://doi.org/10.1177/1363461518799517
Rhemtulla, M., Brosseau-Liard, P. É., & Savalei, V. (2012). When can categorical variables be
treated as continuous? A comparison of robust continuous and categorical SEM
estimation methods under suboptimal conditions. Psychological Methods,
17(3), 354–373. https://doi.org/10.1037/a0029315
Satorra, A., & Bentler, P. M. (2001). A
scaled difference chi‑square test statistic for moment structure
analysis. Psychometrika, 66(4), 507–514. https://doi.org/10.1007/BF02296192
Schumacker, R. E., & Lomax, R. G.
(2010). A beginner’s guide to structural equation modeling (3rd ed.).
Erlbaum.
Tangney, J. P., & Dearing, R. L.
(2002). Shame and guilt. Guilford Press.
Tappenden, P. C., Cole, T. A., Valentine,
J. N., & Lilly, M. M. (2024). Examining the psychometric properties of the
Expressions of Moral Injury Scale in a sample of first responders. Psychological
Trauma: Theory, Research, Practice, and Policy, 16(8), 1319–1328. https://doi.org/10.1037/tra0001569
Weathers, F. W., Litz, B. T., Keane, T. M., Palmieri, P. A., Marx, B. P., & Schnurr, P. P.
(2013). The PTSD Checklist for DSM-5 (PCL-5). National Center
for PTSD.
Wilson, F. R., Pan, W., & Schumsky, D.
A. (2012). Recalculation of the critical values for Lawshe’s content validity
ratio. Measurement and Evaluation in Counseling and Development, 45(3),
197–210. https://doi.org/10.1177/0748175612440286
Wolf, E. J., Harrington, K. M., Clark, S.
L., & Miller, M. W. (2013). Sample Size Requirements for Structural
Equation Models: An Evaluation of Power, Bias, and Solution Propriety. Educational
and psychological measurement, 76(6), 913–934. https://doi.org/10.1177/0013164413495237
LGBT Moral Injury Scale (Spanish version)
Instrucciones: Las siguientes afirmaciones preguntan cómo se
siente respecto de usted mismo/a/e y de su vida. Algunos ítems se refieren a
identidad, relaciones, espiritualidad/religión y valores personales. Indique
cómo se siente ahora mismo frente a cada afirmación, seleccionando un solo
número. No hay respuestas correctas ni incorrectas. Responda todos los ítems.
Escala de respuesta (1–6):
1 = Totalmente en
desacuerdo 4 = Algo
de acuerdo
2 = En desacuerdo 5 =
De acuerdo
3 = Algo en
desacuerdo 6
= Totalmente de acuerdo
|
|
1 |
2 |
3 |
4 |
5 |
6 |
|
1.
Me siento
culpable por no cumplir con las expectativas de mi familia. |
¨ |
¨ |
¨ |
¨ |
¨ |
¨ |
|
2.
Me siento
culpable por no ser heterosexual o cisgénero. |
¨ |
¨ |
¨ |
¨ |
¨ |
¨ |
|
3.
Me siento
culpable por ser quien soy. |
¨ |
¨ |
¨ |
¨ |
¨ |
¨ |
|
4.
Si las personas
supieran mi orientación sexual o identidad de género, tendrían una opinión
más negativa de mí que la que tienen ahora. |
¨ |
¨ |
¨ |
¨ |
¨ |
¨ |
|
5.
Siento vergüenza de mi orientación sexual o identidad de género. |
¨ |
¨ |
¨ |
¨ |
¨ |
¨ |
|
6. Me avergüenza hablar en público sobre mi orientación
sexual o identidad de género. |
¨ |
¨ |
¨ |
¨ |
¨ |
¨ |
|
7.
Por
mis principios, desearía
cambiar mi orientación sexual y/o identidad de género. |
¨ |
¨ |
¨ |
¨ |
¨ |
¨ |
|
8. Desde el punto de vista moral, ser heterosexual y
cisgénero es lo moralmente correcto. |
¨ |
¨ |
¨ |
¨ |
¨ |
¨ |
|
9. Disfruto mi sexualidad, pero reconozco que no es moralmente correcto. |
¨ |
¨ |
¨ |
¨ |
¨ |
¨ |
|
10. Me pregunto qué hice para que Dios me castigue. |
¨ |
¨ |
¨ |
¨ |
¨ |
¨ |
|
11. Siento que Dios me castiga por mi
orientación sexual y/o identidad de género. |
¨ |
¨ |
¨ |
¨ |
¨ |
¨ |
|
12. Me pregunto si Dios me ha abandonado. |
¨ |
¨ |
¨ |
¨ |
¨ |
¨ |
|
13. En ocasiones, me siento inútil. |
¨ |
¨ |
¨ |
¨ |
¨ |
¨ |
|
14. En ocasiones, siento que no sirvo para
nada. |
¨ |
¨ |
¨ |
¨ |
¨ |
¨ |
|
15. En general, me inclino a sentir que soy un
fracaso. |
¨ |
¨ |
¨ |
¨ |
¨ |
¨ |
Note. The authors
of the LGBT Moral Injury Scale hereby place the Spanish version of the
instrument in the public domain to encourage its use in clinical practice and
research. Therefore, no formal permission is required for its reproduction or
use by third parties, beyond appropriate citation of the present article.